
Open Journal of
Clinical and Medical Images
Research Article - Open Access, Volume 4
Promising use of filgotinib in patients affected by systemic sclerosis: Preliminary data from a case series of 5 patients
G Sandri1†; M De Pinto1*†; A Spinella1†; P Macripò1; G Amati1; F Lumetti1; O Secchi1; AF Guerra2; Giuggioli D1,3
1Scleroderma Unit, Chair of Rheumatology, University of Modena and Reggio Emilia, Modena, Italy.
2Internal Medicine and Centre for Hemochromatosis, University Hospital of Modena, University of Modena and Reggio Emilia, Modena, Italy.
3Department of Medical and Surgical Sciences for Children and Adults, University of Modena and Reggio Emilia, Modena, Italy.
*These Authors have Contributed Equally to this Work and Share First Authorship.
*Corresponding Author: Marco De Pinto
Scleroderma Unit, Chair of Rheumatology, University of
Modena and Reggio Emilia, Modena, Italy.
Email: marcodepinto1993@gmail.com
Received : Jan 12, 2024
Accepted : Feb 09, 2024
Published : Feb 16, 2024
Archived : www.jclinmedimages.org
Copyright : © Pinto MD (2024).
Abstract
Objective: To assess the efficacy and safety of Filgotinib for the management of cutaneous, visceral and articular involvement in patients affected by systemic sclerosis.
Methods: 5 patients affected by SSc referring to the Scleroderma Units of Modena and Reggio Emilia between October 2021 and February 2023, were enrolled.
Patients received 200 mg of Filgotinib once daily for a period of 52 weeks. Skin, articular and visceral organ involvement were evaluated at the baseline and every 12 weeks after the start of the treatment.
Results: A significant improvement of articular involvement was seen at 12th week. All patients confirmed a significant amelioration in articular involvement at 52th week, with a significant reduction in TJ, SDAI/CDAI, DAS28-CRP. PDUS performed after 24 and 52 weeks of treatment supported the remission.
A significant decrease of mRSS, improvement of other skin manifestations and a stabilization of ILD, assessed through HRCT and PFTs, were noticed in patients with dcSSc.
The 2 patients with dsSSC showed a clinical improvement assessed using the CRISS score.
No drug-related side effects were recorded and neither patients discontinued the treatment. No deaths were reported.
Conclusion: Filgotinib was safe, effective and well tolerated in the treatment of articular and visceral involvement in patients affected by SSc.
Keywords: Filgotinib; JAK inhibitors; Rheumatoid arthritis; Systemic sclerosis.
Citation: Sandri G, Pinto MD, Spinella A, Macripò P, Amati G, et al. Promising use of filgotinib in patients affected by systemic sclerosis: Preliminary data from a case series of 5 patients. Open J Clin Med Images. 2024; 4(1): 1165.
Introduction
Systemic Sclerosis (SSc) is a Connective Tissue Disease (CTD) characterised by endothelial dysfunction, vasculopathy and dysregulation of the immune system, resulting in fibrosis of the skin and internal organs.
SSc pathogenesis is complex and involves a pleiotropic pool of cell types, cytokines, growth factors and signalling pathways, displaying both inflammatory and fibrotic processes as pathological hallmarks [1].
The quality of life of SSc patients is commonly impaired by the development of progressive skin fibrosis and Interstitial Lung Disease (ILD) and mortality related to the disease, in particular due to cardio-pulmonary causes, remains significant [2].
In the past years, several drugs were studied for SSc [3-9]. Scleroderma Lung Study (SLS) I [3], confirmed the efficacy of cyclophosphamide on lung function and health-related symptoms in patients with SSc-ILD, and SLS II [4] further highlighted that Mycophenolate Mophetile (MMF) have a comparative, but not superior, effect on lung function, dyspnea, lung imaging, and skin disease with a better tolerance. In the recent years, the faSScinate RCT on the use of Tocilizumab in SSc, concluded that Tocilizumab might preserve lung function in people with early SSc-ILD and elevated acute phase reactants [5]. Similarly, Nintedanib, a Tyrosine Kinase Inhibitor, was approved for treatment of SSc-ILD, based on the results of the SENSCISS trial [6]. More recently, INBUILD trial investigated the efficacy and safety of Nintedanib versus placebo in patients with progressive fibrosing ILDs, including SSc-ILD, confirming the efficacy in slowing the rate of decline in FVC [7,8]. At last, recently published results of the RECITAL trial showed that Rituximab should be considered a therapeutic alternative to cyclophosphamide in individuals with CTD-ILD [9].
Despite new agents being currently available for treatment of SSc, none of these have been proved to be effective for fibrotic skin involvement. Moreover, standard therapy is often inadequate and hampered by side effects. Therefore, SSc treatment still must be considered an unmet need.
Targeting multiple cytokines might be an innovative therapeutic strategy as opposed to single-cytokine bDMARDs, which have been proved to be ineffective.
Janus Kinases (JAKs) are protein Tyrosine Kinases (TYKs) involved in several biological processes, such as cellular proliferation and differentiation, apoptosis and fibrogenesis, modulating cellular responses to many cytokines and growth factors. There is growing evidence that JAK/STAT signalling pathways may play a crucial role in SSc pathogenesis. JAK-inhibitors (JAKi) could therefore be considered a new potential treatment for SSc [10].
The aim of our work was to assess efficacy and safety of Filgotinib, a highly selective JAK1 inhibitor, for the management of cutaneous, visceral, and articular involvement in patients affected by SSc.
Material and methods
Prospective, open-label, monocentric study in which 5 patients affected by SSc referring to the Scleroderma Units of Modena and Reggio Emilia between October 2021 and February 2023, were enrolled. All patients satisfied ACR/EULAR criteria for SSc [11].
All patients were >18 years old and were already under treatment with standard therapy (prostanoids, calcium-channel blockers a/o endothelin-receptors inhibitors a/o phosphodiesterase type 5 inhibitors) and had an inadequate response or were intolerant or had contraindication to one or more Disease-Modifying Anti-Rheumatic Drugs (DMARDs) or biologicalDMARDs (bDMARDs).
At the beginning of the treatment with Filgotinib, the patients showed one or more active SSc clinical manifestations which had been scarcely responsive to previous and/or ongoing treatments (Table 1).
Patients received 200 mg of Filgotinib once daily for a period of 52 weeks.
Exclusion criteria were pregnant or breastfeeding women; age <18 years old; current or prior history of treatment within the 3 months prior to baseline with (bDMARDs); contraindication to the use of Filgotinib, including neutropenia (ANC<1x109 cells/L), lymphopenia (ALC<0,5x109 cells/L), anaemia (Hb<8 g/ dl), end-stage renal disease (CrCl<15ml/min), severe hepatic impairment (Child-Pugh C), current serious infection. In addition, patients with history of malignancy in the last 5 years were excluded.
Skin, articular, visceral organ involvement, including pulmonary, cardiac, renal, and gastrointestinal alterations, as well as routine blood chemistry and autoimmunity were evaluated according to clinical practice [12,13]. Adverse events attributable to Filgotinib were also recorded.
Articular involvement
Articular involvement was assessed trough clinical evaluation of number of Tender and Swollen Joints (TJ/SJ), the Numeric Rating Scale (NRS, 0-10) and the use of composite activity indexes, including modified Disease Activity Score that includes 28 different joint counts (DAS28) [14], Clinical Disease Activity Index (CDAI) and Simplified Disease Activity Index (SDAI), at the baseline and after 3, 6 and 12 months of treatment.
Power Doppler Ultrasonographic (PDUS) examination evaluated the presence of active synovitis, power Doppler signal, and synovial hypertrophy on the following bilateral joints: metacarpophalangeal-proximal interphalangeal joints-flexor and extensor tendons and wrist (radiocarpal and midcarpal joints). US was carried-out by trained physician, in a blinded fashion using a multi-frequency linear probe (10-18 MHz) at the baseline, the end of follow-up and every time there was a clinical suspect of synovitis and tenosynovitis.
Skin involvement
The extent of skin thickening was evaluated by the Modified Rodnan Skin Score (mRSS), performed by an experienced physician evaluated, in a blinded fashion, at the baseline and after 3, 6 and 12 months of Filgotinib treatment. Skin assessment was carried out every time by the same physician and included the presence and severity of Digital Ulcers (DUs), melanoderma, pruritus, skin tightening, telangiectasias and calcinosis.
Nailfold videocapillaroscopy was performed at the baseline in all patients.
Cardiac and pulmonary involvement
The presence of ILD was identified on the basis of a HighResolution Computed Tomographic scan (HRCT), obtained within 12 months before screening, which showed fibrosis affecting at least 10% of the lungs, as confirmed by an expert radiologist, according to SENSCIS trial [6].
Pulmonary Function Tests (PFTs), namely, Total Lung Capacity (TLC), Forced Vital Capacity (FVC), Diffusing capacity of the Lungs for Carbon monoxide (DLCO), 6-minute walking test and trans-thoracic Echo-Color-Doppler Cardiography (ECHOcg), were performed in all patients at baseline, after 6 months of Filgotinib treatment, and at the end of follow-up. HCRT was repeated after 12 months of treatment. Rating of perceived exertion was evaluated by means of Modified Borg Dyspnoea Scale at baseline and every 3 months.
The presence of PAH, defined by the presence pulmonary artery pressure (mPAP) >20 mmHg at rest, measured by Right Heart Catheterization (RHC), with a Pulmonary Capillary Wedge Pressure (PCWP) ≤15 mmHg, and a Pulmonary Vascular Resistance (PVR) ≥3 Wood units, was not considered an exclusion criterion.
Quality of life assessment
The Health Assessment Questionnaire-Disability Index (HAQDI) was administrated at baseline, at the 6th month of treatment and at the end of follow-up to assess patients’ quality of life. Numeric Rating Scale for pain (NRS) was reported before to start the treatment and every 3 months.
ACR CRISS score
The American College of Rheumatology (ACR) Composite Response Index In Dcssc (CRISS) score is a novel composite index developed for use in clinical trials to assess whether new pharmacologic agents have an impact on overall disease activity/severity [15].
The ACR CRISS score is a continuous variable between 0.0 and 1.0, which define the probability of improving after 12 months of treatment, using a probability cut-off of 0.6.
It is applied in 2 steps:
- In the 1st step, patients who develop new onset of renal crisis, new onset or worsening of ILD (defined by decline in FVC predicted ≥15%, confirmed by another FVC% within a month), new onset of PAH, or new onset of left ventricular failure during the trial are considered as not improved and assigned a probability of improving equal to 0.0;
- In the 2nd step, the predicted probability of improving for each remaining patients, is calculated through an equation, which includes the mean changes from baseline of 5 items assessed at 52th week; mRSS, FVC (%), Patient Global Assessment (PTGA) of Overall Health (NRS 0-10), Physician Global Assessment (MDGA) of Overall Health (NRS 0-10), and HAQ-DI.
Data analysis was carried out using the SPSS statistical package (version 26.0, IBM Software, USA). Comparisons between values were performed using the ANOVA test and Fisher’s exact test for continuous and noncontinuous variables, respectively. All descriptive data are expressed as mean ± Standard Deviation (SD). p values ≤ 0.05 were considered statistically significant.
Table 1: Demographic and clinical-epidemiological features of SSc patients.
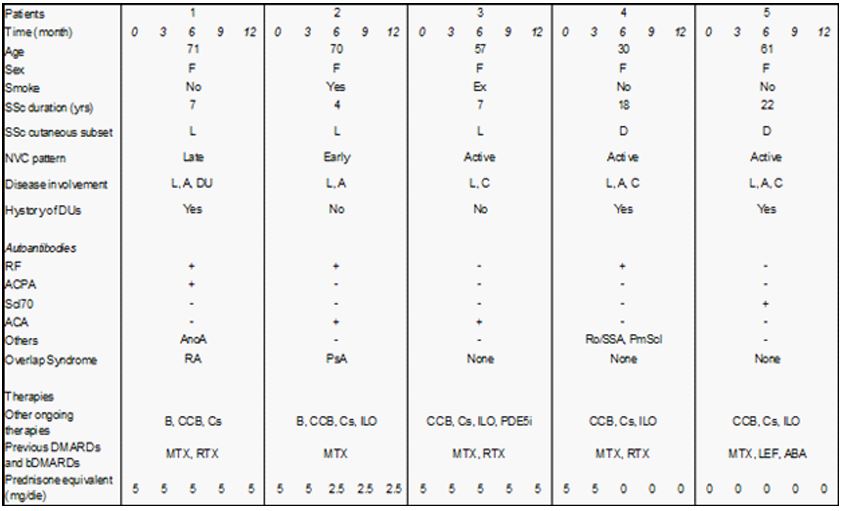
Table 2: Articular and cutaneous features of SSc patients treated with Filgotinib.
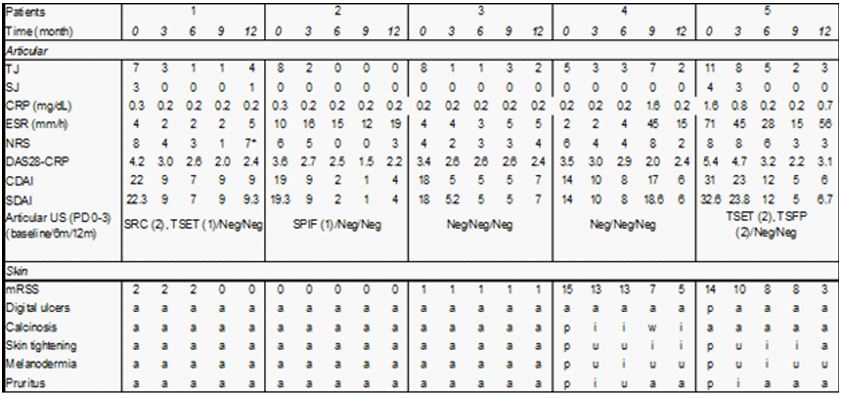
Table 3: Cardio-pulmonary features and CRISS score of SSc patients treated with Filgotinib.
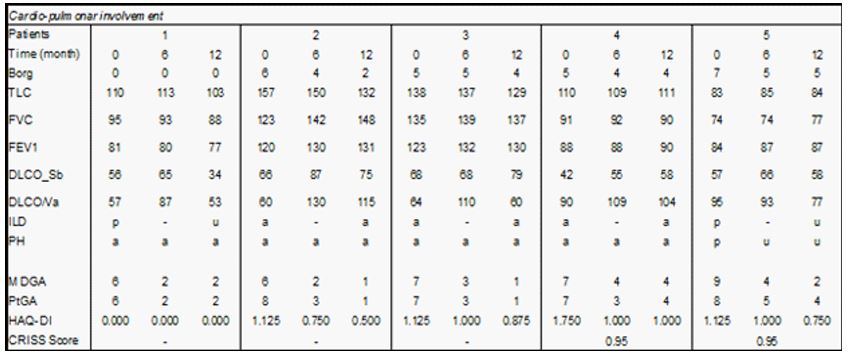
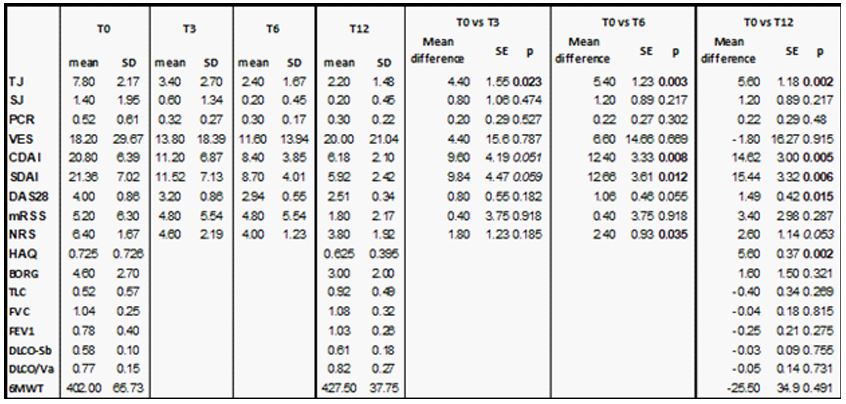
Table 4: Clinical assessment of our SSc population during follow-up: statistical comparisons from baseline (T0) to 12 weeks (T3), 24 weeks (T6) and 52 weeks (T12) after treatment with Filgotinib.
Results
Demographic and clinical-epidemiological features of enrolled patients are shown in Table 1. All patients were female (M/F 0/5), with median age 57,80±16,62 DS years and disease duration of 11,6±7,89 DS years. 3 patients presented a limited cutaneous subset and 2 patients a diffuse subset. Serum ACA were detected in 2 subjects, circulating anti Scl-70 in one, ANoA, Pm-Scl and SSA in one, rheumatoid factor in 3. One patient had been diagnosed with an overlap syndrome with RA and one patient with PsA.
Moreover, 2 patients displayed ILD, 1 patient had mixed PH (precapillary and postcapillary PH, in the context of ILD), 1 patient had calcinosis and 3 patients had a history of recurrent DUs, in one patient complicated by osteomyelitis and acrosteolysis.
Three patients had previously been treated with rituximab and 2 with abatacept, which were suspended due to adverse reactions or inefficacy. All patients had been treated with methotrexate, which was discontinued in 3 patients for gastrointestinal intolerance, 1 patient had been treated with leflunomide, suspended for inefficacy, and 3 patients were being treated with hydroxychloroquine sulphate. 4 patients were taking low dose of steroids (5 mg of prednisone equivalent).
All patients showed a significant improvement in articular involvement (Table 2). At the baseline, 4 patients displayed a moderate disease activity and one patient a high disease activity according to DAS28-CRP (3,99±0,86) and SDAI/CDAI (21,36±7,02 and 20,80±6,39 respectively).
Notably, a significant reduction in TJ (p=0,023) and a trend of improvement of SDAI/CDAI (p=0,059/0,051) had already been noticed at 12th week, which became significant after 24 weeks (SDAI p=0,12, CDAI p=0,008, Table 4). After 52 week of treatment a significant reduction in TJ (from 7,80±2,17 to 2,20±1,48, p=0,002), CDAI (from 20,80±6,39 to 6,18±2,10, p=0,005), SDAI (from 21,36±7,02 to 5,92±2,42, p=0,006) and DAS28-CRP (from 3,99±0,86 to 2,51±0,34, p=0,015) (Table 4).
According to DAS28-RCP, 80% of the patients (4/5), were in remission and 1 patient had a low disease activity at the end of follow-up.
A significant improvement of NRS was observed after 24 weeks of treatment (from 6,40±1,67 to 4,00±1,23, p=0,03), and a trend of improvement was confirmed at 52th week (3,80±1,92, p=0,053, Table 4). Also a significant reduction of HAQ (from 0,725±0,726 to 0,625±0,395, p=0,002), was seen after 52 weeks (Table 4).
A mild reduction without significant differences was noted in CRP (0,52±0,61 to 0,30±0,22, p=0,48) and ESR (18,20±29,67 to 20,00±21,04, p=0,915) after 52 weeks of treatment (Table 4).
PDUS assessment at the baseline revealed the presence of active synovitis of radiocarpal joint, proximal inter-phalangeal joints and tenosynovitis of flexor and extensor tendons in 3 patients (Table 2). PDUS performed after 6 and 12 months of treatment confirmed the absence of synovitis and tenosynovitis in all patients.
The extent and severity of skin involvement assessed through mRSS remained stable during follow-up (from 5,20±6,30 to 1,80±2,17 at 52th week, p=0,287, Table 2 and 4).
However, both patients with dcSSc showed an important clinical improvement of SSc skin manifestations. In particular a marked reduction of mRSS at 52th week, 10 (from 15 to and 5) and 11 points (from 14 to 3) respectively, was observed (Table 2). Similarly, a valuable improvement of other skin manifestations, namely melanoderma, pruritus and skin tightening had already been noticed after 24 weeks in patients with dcSSc, (Table 2). No patients developed DUs, even patients with a history of recurrent DUs.
Regarding cardio-pulmonary involvement (Table 3), no differences were observed in PFTs, namely FVC (p=0,815), TLC (p=0,269), DLCO (Sb p=0,755; Va=0,731) and during the 6 minute walking test (p=0,491) and exertional dyspnea, measured using the Borg scale (from 4.60±2.70 to 3.00±2.00, p=0.321) as shown in Table 4. In the 2 patients with ILD, HRCT performed after 12 months showed an unchanged involvement.
Both subjects with dsSSC showed a clinical improvement defined by a CRISS score of 0.95, with an improvement in 4/5 items (HAQ, MDGA, PtGA and mRSS) and no worsening of FVC (Table 3).
No severe drug-related side effects were recorded during follow-up and none of the patients discontinued the treatment. Notably no patients experienced adverse cardiovascular events or worsening of PH, evaluated through reported symptoms and echocardiographic parameters. No deaths were reported.
Discussion
The results of the present study seem to support the safety and efficacy of Filgotinib for the management of articular and visceral involvement in SSc.
Despite the availability of several new agents, SSc treatment must still be considered as an unmet need. The efficacy of standard immunosuppressive therapies is currently limited, and no drugs have proved to be effective for fibrotic skin involvement. Moreover, drug-related side effects are common and often limit the use of newer molecules.
Compared to single-target drugs, Filgotinib has a wider spectrum of action, by modulating several cytokine receptors, implicated in inflammation and fibrogenic processes [16].
In our population the greater effectiveness was seen on articular involvement. An initial clinical effect had already been noticed after 12 weeks and a significant improvement with both reduction of TJ and SJ and an improvement of CDAI, SDAI and DAS28-CRP, was confirmed after 52 weeks of treatment. According to DAS28-CRP, 80% of our patients obtained remission of articular disease at the end of the follow-up. Moreover, the absence of subclinical inflammation was confirmed with PDUS after 6 and 12 months of treatment.
At the end of the follow-up, a considerable improvement of quality of life, defined by a reduction of HAQ, had also been observed.
Filgotinib treatment also led to a significant reduction of mRSS in patients with diffuse cutaneous subset. A concomitant clinically significant improvement of symptoms related to cutaneous disease activity, namely melanoderma, pruritus, skin tightening was observed. No patients developed DUs during follow-up, even in patients with a history of recurrent DUs, acrosteolysis and amputations. A stabilization of ILD detected in 2 patients, assessed through HRCT and PFTs, was observed. Finally, an overall clinical improvement in patients with dcSSc was confirmed by the CRISS score.
Filgotinib is an oral second-generation preferential JAK1 inhibitor, already approved for use in Europe, UK and Japan for the treatment of Rheumatoid Arthritis (AR) and Ulcerative Colitis (UC) [16] on the basis of the results of FINCH [17] and SELECTION trial [18], respectively. It also displayed a promising clinical profile in the FITZROY study [19] in patients with Crohn Disease (CD) and TORTUGA study [20] in patients with SpA.
In biochemical assays, Filgotinib demonstrated an high selective inhibition profile for JAK1 and showed >5-fold higher potency for JAK1 over JAK2, JAK3, and tyrosine kinase. In vitro assay also showed that Filgotinib inhibited erythroid progenitor expansion, carried out by JAK2 through GM-CSF, less potently than the other JAKi [10]. This may explain the better safety profile in relation to the laboratory abnormalities observed in the trials conducted for RA patients [21].
JAK1 is fundamental for the signalling of several cytokines, namely IL-6, IL-2, IL-4, IL-10, IL-11, IL-19, IL-20, IL-22, and Interferon (IFN) alpha, IFN-beta, and IFN-gamma, which play a key role in inflammatory and fibrogenic processes [10].
There is growing evidence that JAK/STAT pathway plays a pivotal role in SSc pathogenesis [22]. Recent in vitro studies have shown that the JAK/STAT pathway is activated in SSc and JAKi are effective in modulating inflammation and fibrogenic process, acting on mesenchymal and epithelial cells, lymphocytes and macrophages [23-25]. JAKi exhibit both anti-inflammatory and anti-fibrotic properties, linked to the modulation of the activation state of pro-inflammatory M1 macrophages, but also limiting M2a activation of macrophages [23,26].
Therefore, JAK/STAT appears to be relevant therapeutic target to evaluate in potential treatments for SSc.
To our knowledge, this is the first description of Filgotinib use in SSc.
Descriptions of JAKi usage for SSc in clinical practice are sparse and characterized by heterogeneity of population and low quality of evidences. In particular, descriptions are limited to few case reports [27-33], one single-center, open-label clinical trial [34], one pilot study [35] and a prospective observational study [36]. A total of 60 SSc patients were globally recruited in these studies, 2 of whom with defined overlap syndrome with RA [28,29] and one with SpA [30].
The presence of articular involvement represents the main indication for the use of Filgotinib in our study, and for the use of JAKi in general in patients with SSc [28-31,35,37]. This is not surprising considering the established role of Filgotinib in RA [17].
The main study on the use of JAKi in SSc, in a pilot study performed by Karalilova et al. in 2021 [35]. They compared treatment regimen with methotrexate and JAKi in 66 scleroderma patients, randomized in two arms. After 52 weeks of treatment, JAKi demonstrated greater efficacy than methotrexate in the improvement of musculoskeletal involvement, assessed through US in 10 joints.
The efficacy of Filgotinib in RA can mainly be explained by its anti-inflammatory action, through the inhibition of IL-6 and IFN type I signaling. Moreover, in vitro studies demonstrate that Filgotinib dosage dependently inhibits Th1 and Th2 differentiation, and limits, to a lower degree, the differentiation of Th17 cells [38].
Other than the aforementioned anti-inflammatory effects, JAKi also displayed anti-fibrotic properties, making its use challenging in fibrosing diseases [23].
Indeed, several in vitro studies on SSc patients and murine fibrotic model have shown that JAKi could be effective in ameliorating or preventing fibrogenesis, by modulating inflammation and the fibrogenic process, acting on mesenchymal and epithelial cells, lymphocytes and macrophages [23-25,39-42].
Interestingly, Karalilova et al. had also observed a greater reduction of mRSS and skin thickness, assessed through US in 5 anatomical sites, and a significantly lower number of cumulative DUs in the JAKi arm than methotrexate one [35]. Globally, a significant cutaneous response (decrease in the mRSS of >5 points and ≥25% from baseline) was reported in 88% (52 patients) of the scleroderma patients treated with JAKi [43]. An improvement of “salt and pepper” skin and digital ulcers was also described [27,33].
Indeed, the results of the present study seem to confirm the poor data from the literature, especially regarding the treatment of skin and articular involvement. In the present work, the improvement of skin sclerosis and skin disease related symptoms was clearly observed in patients with dcSSc.
Remarkably, in our small cohort of patients a functional and radiological stabilization of ILD, assessed through PFTs and HRCT, and a significant improvement of dyspnea, has been observed.
Despite the development, over the last two decades, of a wide range of biological therapies, SSc-ILD still represents a major cause of death in scleroderma patients [2,13].
Based on the first RCTs in scleroderma-ILD [3,4] cyclophosphamide is the accepted standard of care with micophenolate mofetil for individuals with severe or progressive CTD-related ILD. More recently, RCTs for the use of Tocilizumab [5] and Rituximab [9] have shown positive effect in the management of SSC-ILD. Finally, Nintedanib, a Tyrosine Kinase Inhibitor, has been approved for treatment of SSc-ILD, based on the results of the SENSCISS and INBUILD trial [6-8]. However the overall efficacy of new therapies is limited, and side effects may be common and debilitating.
JAKi could represent a pioneering treatment for SSc-ILD due to combined anti-fibrotic and anti-inflammatory properties that have been showed in vivo and in vitro [23].
In fact, JAKi and Filgotinib have already demonstrated to be a safe therapeutic option for the management of RA-associated ILD [44].
Finally, a recent literary review on the use of JAKi for the treatment of SSc-ILD [37] concluded that JAKi might lead to stabilisation or improvement of SSc-ILD in the majority of cases, with the exception of only 2 cases reporting a worsening of ILD. Nevertheless, it is usually well tolerated, with no cardiovascular events described in any study.
Considering PH, some authors discussed recent novel targets of therapies that have been developed, however, these are still in a pre-clinical phase and RCTs are clearly not available. While in recent years substantial progress has been made in targeting key molecular pathways, PH still remains without a definitive cure, and these novel therapies provide an important conceptual framework for categorizing patients on the basis of molecular phenotypes and subsets for effective treatment of the disease [45].
Some recent studies have also suggested that JAK/STAT pathway could be targeted for treating Pulmonary Arterial Hypertension (PAH), a severe and frequent SSc complication [46,47], although evidences are controversial [48-50].
In the present work no patients of our cohort experienced worsening of pre-existing PH.
Moreover, despite the recent FDA warning regarding the increased risk of major adverse cardiovascular events, malignancy, thrombosis and mortality correlated with the use of JAKi, no events were reported during the follow-up. Preferential inhibition of JAK1 modulates a subset of proinflammatory cytokines, which differ from those inhibited by JAK2 or JAK3 and could explain the favorable safety profile of Filgotinib compared to pan-JAKi [10,16]. Nevertheless, evaluation of cardiovascular risk factors is strongly suggested for patients applying for Filgotinib therapy.
Evaluation of drug efficacy may be challenging in SSc due to the heterogeneity of skin and organ involvement, as well as the lack of well-assessed disease activity scale. Therefore, the American College of Rheumatology (ACR) has recently proposed the CRISS score as a new composite response index to assess the likelihood of improvement in patients with dcSSc after 52 weeks of treatment with new pharmacologic agents [15]. In the present study a clinical improvement, defined CRISS score >0.6, was confirmed in the patients with dcSSc.
Conclusion
According to our preliminary data, Filgotinib was safe, effective and well tolerated in the treatment of articular, skin and visceral involvement in patients affected by SSc. The greater effectiveness was observed in the management of articular manifestations, which had already been detected after 12 weeks of treatment. A promising improvement of skin involvement, stabilization of ILD and overall clinical improvement defined by the CRISS score, had also been observed in patients with dcSSc. An improvement of the quality of life, defined by a reduction of HAQ, was also reported at the end of the follow-up.
Safety profile was satisfactory and no worsening of PH or cardiovascular events were reported.
Despite the limitations of our preliminary study, namely the small sample size and heterogeneity of the patients with a long standing disease and multi-failure to treatment, the use of Filgotinib in SSc is challenging, yet promising.
Further analysis on a larger number of patients and control group are needed to confirm our data, since no RCT is available at the moment. If confirmed, JAKi - namely Filgotinib - could represent a new horizon in the management of such a complex disease, which currently still lacks a satisfactory treatment.
Declarations
Written informed consent and ethic committee: The study was approved by the local ethics committee Area Vasta Emilia Nord (protocol no. 275/16), and written informed consent was obtained from all participants. The study was performed in accordance with the Good Clinical Practice Guidelines and with the World Medical Association Declaration of Helsinki, revised in 2000, Edinburgh.
Conflict of interests: Authors state that they have no conflict of interest to declare.
Ethics approval: The study was approved by the local ethics committee Area Vasta Emilia Nord (protocol no. 275/16). The study was performed in accordance with the Good Clinical Practice Guidelines and with the World Medical Association Declaration of Helsinki, revised in 2000, Edinburgh.
Acknowledgements: Not applicable.
References
- Denton CP, Khanna D. Systemic sclerosis. The Lancet. Lancet Publishing Group; 2017; 390: 1685-99.
- Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972-2002. Ann Rheum Dis. 2007; 66(7): 940-4.
- Tashkin DP, Elashoff R, Clements PJ, Goldin J, Roth MD, et al. Cyclophosphamide versus placebo in scleroderma lung disease. N Engl J Med. 2006; 354(25): 2655-66. Available from: https: //pubmed.ncbi.nlm.nih.gov/16790698/
- Tashkin DP, Roth MD, Clements PJ, Furst DE, Khanna D, et al. Mycophenolate Mofetil versus Oral Cyclophosphamide in Scleroderma-related Interstitial Lung Disease: Scleroderma Lung Study II (SLS-II), a double-blind, parallel group, randomised controlled trial. Lancet Respir Med [Internet]. 2016 Sep 1 [cited 2023 Apr 11]; 4(9): 708. Available from: /pmc/articles/PMC5014629/
- Khanna D, Lin CJF, Furst DE, Goldin J, Kim G, et al. Tocilizumab in systemic sclerosis: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2020; 8(10): 963-74.
- Distler O, Highland KB, Gahlemann M, Azuma A, Fischer A, et al. Nintedanib for Systemic Sclerosis-Associated Interstitial Lung Disease. New England Journal of Medicine. 2019; 380(26): 2518-28.
- Wells AU, Flaherty KR, Brown KK, Inoue Y, Devaraj A, et al. Nintedanib in patients with progressive fibrosing interstitial lung diseases-subgroup analyses by interstitial lung disease diagnosis in the INBUILD trial: A randomised, double-blind, placebo-controlled, parallel-group trial. Lancet Respir Med. 2020; 8(5): 453-60. Available from: https: //pubmed.ncbi.nlm.nih.gov/32145830/
- Matteson EL, Kelly C, Distler JHW, Hoffmann-Vold AM, Seibold JR, et al. Nintedanib in Patients With Autoimmune Disease–Related Progressive Fibrosing Interstitial Lung Diseases: Subgroup Analysis of the INBUILD Trial. Arthritis and Rheumatology. 2022; 74(6): 1039-47.
- Maher TM, Tudor VA, Saunders P, Gibbons MA, Fletcher S V, et al. Rituximab versus intravenous cyclophosphamide in patients with connective tissue disease-associated interstitial lung disease in the UK (RECITAL): a double-blind, double-dummy, randomised, controlled, phase 2b trial. Lancet Respir Med [Internet]. 2023; 11(1): 45-54. Available from: https: //pubmed.ncbi.nlm.nih.gov/36375479/
- Traves PG, Murray B, Campigotto F, Galien R, Meng A, et al. JAK selectivity and the implications for clinical inhibition of pharmacodynamic cytokine signalling by filgotinib, upadacitinib, tofacitinib and baricitinib. Ann Rheum Dis. 2021; 80(7): 865-75. Available from: https: //pubmed.ncbi.nlm.nih.gov/33741556/
- Van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013; 65(11): 2737-47. Available from: https: //pubmed.ncbi.nlm.nih.gov/24122180/
- Ferri C, Valentini G, Cozzi F, Sebastiani M, Michelassi C, et al. Systemic sclerosis: Demographic, clinical, and serologic features and survival in 1,012 Italian patients. Medicine [Internet]. 2002; 81(2): 139-53. Available from: https: //pubmed.ncbi.nlm.nih.gov/11889413/
- Ferri C, Sebastiani M, Lo Monaco A, Iudici M, Giuggioli D, et al. Systemic sclerosis evolution of disease pathomorphosis and survival. Our experience on Italian patients’ population and review of the literature. Autoimmun Rev. 2014; 13(10): 1026–34. Available from: https: //pubmed.ncbi.nlm.nih.gov/25182204/
- Prevoo MLL, Van’T Hof MA, Kuper HH, van Leeuwen MA, van de Putte LBA, et al. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995; 38(1): 44-8. Available from: https: //pubmed.ncbi.nlm.nih.gov/7818570/
- Khanna D, Berrocal VJ, Giannini EH, Seibold JR, Merkel PA, et al. The American College of Rheumatology Provisional Composite Response Index for Clinical Trials in Early Diffuse Cutaneous Systemic Sclerosis. Arthritis Rheumatol. 2016; 68(2): 299-311. Available from: https: //pubmed.ncbi.nlm.nih.gov/26808827/
- Namour F, Anderson K, Nelson C, Tasset C. Filgotinib: A Clinical Pharmacology Review. Clin Pharmacokinet. 2022; 61(6): 819-32. Available from: https: //pubmed.ncbi.nlm.nih.gov/35637376/
- Genovese MC, Kalunian K, Gottenberg JE, Mozaffarian N, Bartok B, Matzkies F, et al. Effect of Filgotinib vs Placebo on Clinical Response in Patients With Moderate to Severe Rheumatoid Arthritis Refractory to Disease-Modifying Antirheumatic Drug Therapy: The FINCH 2 Randomized Clinical Trial. JAMA. 2019; 322(4): 315-25. Available from: https: //pubmed.ncbi.nlm.nih.gov/31334793/
- Feagan BG, Danese S, Loftus EV, Vermeire S, Schreiber S, et al. Filgotinib as induction and maintenance therapy for ulcerative colitis (SELECTION): A phase 2b/3 double-blind, randomised, placebo-controlled trial. Lancet. 2021; 397(10292): 2372-84.Available from: https: //pubmed.ncbi.nlm.nih.gov/34090625/
- Vermeire S, Schreiber S, Petryka R, Kuehbacher T, Hebuterne X, et al. Clinical remission in patients with moderate-to-severe Crohn’s disease treated with filgotinib (the FITZROY study): Results from a phase 2, double-blind, randomised, placebo-controlled trial. Lancet. 2017; 389(10066): 266-75. Available from: https: //pubmed.ncbi.nlm.nih.gov/27988142/
- Van der Heijde D, Baraliakos X, Gensler LS, Maksymowych WP, Tseluyko V, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active ankylosing spondylitis (TORTUGA): results from a randomised, placebo-controlled, phase 2 trial. Lancet. 2018; 392(10162): 2378-87. Available from: https: //pubmed.ncbi.nlm.nih.gov/30360970/
- Fragoulis GE, Mcinnes IB, Siebert S. JAK-inhibitors. New players in the field of immune-mediated diseases, beyond rheumatoid arthritis. Rheumatology (Oxford). 2019; 58(Suppl 1): i43-54. Available from: https: //pubmed.ncbi.nlm.nih.gov/30806709/
- Raja J, Denton CP. Cytokines in the immunopathology of systemic sclerosis. Seminars in Immunopathology. 2015; 37(5): 543-57. Available from: https: //link.springer.com/article/10.1007/s00281-015-0511-7
- Lescoat A, Lelong M, Jeljeli M, Piquet-Pellorce C, Morzadec C, et al. Combined anti-fibrotic and anti-inflammatory properties of JAK-inhibitors on macrophages in vitro and in vivo: Perspectives for scleroderma-associated interstitial lung disease. Biochem Pharmacol. 2020; 178.
- Kitanaga Y, Imamura E, Nakahara Y, Fukahori H, Fujii Y, et al. In vitro pharmacological effects of peficitinib on lymphocyte activation: A potential treatment for systemic sclerosis with JAK inhibitors. Rheumatology (United Kingdom). 2020; 59(8).
- Wang H, Feng X, Han P, Lei Y, Xia Y, et al. The JAK inhibitor tofacitinib ameliorates immune mediated liver injury in mice. Mol Med Rep. 2019; 20(6).
- Chen H, Li M, Sanchez E, Soof CM, Bujarski S, et al. JAK1/2 pathway inhibition suppresses M2 polarization and overcomes resistance of myeloma to lenalidomide by reducing TRIB1, MUC1, CD44, CXCL12, and CXCR4 expression. Br J Haematol. 2020; 188(2).
- Deverapalli SC, Rosmarin D. The use of JAK inhibitors in the treatment of progressive systemic sclerosis. Vol. 32, Journal of the European Academy of Dermatology and Venereology. 2018.
- Fujita Y, Nawata M, Nagayasu A, Someya K, Saito K, et al. FiftyTwo-Week Results of Clinical and Imaging Assessments of a Patient with Rheumatoid Arthritis Complicated by Systemic Sclerosis with Interstitial Pneumonia and Type 1 Diabetes despite Multiple Disease-Modifying Antirheumatic Drug Therapy That Was Successfully Treated with Baricitinib: A Novel Case Report. Case Rep Rheumatol. 2019; 2019.
- Boleto G, Cren JB, Avouac J, Allanore Y. Successful treatment with baricitinib of refractory arthritis in a patient with severe diffuse cutaneous systemic sclerosis-rheumatoid arthritis overlap syndrome. Clin Exp Rheumatol . 2021; 39: 163-4.
- Kyriakou A, Parperis K, Nikiphorou E, Psarelis S. Successful use of tofacitinib in the treatment of diffuse systemic sclerosis and axial spondyloarthritis: a case-based review. Rheumatology International. 2021; 41.
- Komai T, Shoda H, Hanata N, Fujio K. Tofacitinib rapidly ameliorated polyarthropathy in a patient with systemic sclerosis. Scand J Rheumatol. 2018; 47(6): 505-6. Available from: https: //pubmed.ncbi.nlm.nih.gov/29260607/
- Troncoso JÁ, González AN, Robles EM, Torre RS, Marhuenda ÁR. Tofacitinib Is an Effective Treatment for Refractory Scleromyositis Associated With Anti-PM/Scl. Cureus. 2023; 15(1). Available from: /pmc/articles/PMC9947514/
- Nallapati A, Wigley FM, Paik JJ. Improvement of salt and pepper skin changes in diffuse scleroderma after treatment with tofacitinib. Clin Exp Rheumatol. 2022; 40(10): 2008-9. Available from: https: //pubmed.ncbi.nlm.nih.gov/36189907/
- You H, Xu D, Hou Y, Zhou J, Wang Q, et al. Tofacitinib as a possible treatment for skin thickening in diffuse cutaneous systemic sclerosis. Rheumatology (United Kingdom). 2021; 60(5).
- Karalilova RV, Batalov ZA, Sapundzhieva TL, Matucci-Cerinic M, Batalov AZ. Tofacitinib in the treatment of skin and musculoskeletal involvement in patients with systemic sclerosis, evaluated by ultrasound. Rheumatol Int. 2021; 41(10).
- Hou Z, Su X, Han G, Xue R, Chen Y, et al. JAK1/2 Inhibitor Baricitinib Improves Skin Fibrosis and Digital Ulcers in Systemic Sclerosis. Front Med (Lausanne). 2022; 9.
- Fiorentini E, Bonomi F, Peretti S, Orlandi M, Lepri G, Matucci Cerinic M, et al. Potential Role of JAK Inhibitors in the Treatment of Systemic Sclerosis-Associated Interstitial Lung Disease: A Narrative Review from Pathogenesis to Real-Life Data. Life. MDPI. 2022; 12.
- Raimondo MG, Biggioggero M, Coletto LA, Ramming A, Caporali R, et al. Clinical pharmacology of filgotinib in the treatment of rheumatoid arthritis: current insights. Expert Rev Clin Pharmacol. 2021; 14(6): 661-70. Available from: https: //pubmed.ncbi.nlm.nih.gov/33847204/
- Damsky W, Patel D, Garelli CJ, Garg M, Wang A, et al. Jak Inhibition Prevents Bleomycin-Induced Fibrosis in Mice and Is Effective in Patients with Morphea. Journal of Investigative Dermatology. 2020; 140(7).
- Wang W, Bhattacharyya S, Marangoni RG, Carns M, Dennis-Aren K, et al. The JAK/STAT pathway is activated in systemic sclerosis and is effectively targeted by tofacitinib. J Scleroderma Relat Disord. 2019; 41. Al-Fayoumi S, Hashiguchi T, Shirakata Y, Mascarenhas J, Singer JW. Pilot study of the antifibrotic effects of the multikinase inhibitor pacritinib in a mouse model of liver fibrosis. J Exp Pharmacol. 2018; 10.
- Sendo S, Saegusa J, Yamada H, Nishimura K, Morinobu A. Tofacitinib facilitates the expansion of myeloid-derived suppressor cells and ameliorates interstitial lung disease in SKG mice. Arthritis Res Ther. 2019; 21(1).
- Moriana C, Moulinet T, Jaussaud R, Decker P. JAK inhibitors and systemic sclerosis: A systematic review of the literature. Autoimmun Rev. 2022; 21(10). Available from: https: //pubmed.ncbi.nlm.nih.gov/35944611/
- Garton M, Kelly C. Is Janus Kinase Inhibition the Future of the Management of Rheumatoid Arthritis-associated Interstitial Lung Disease? US Respir Pulm Dis. 2022; 7(2): 38.
- Hu J, Xu Q, McTiernan C, Lai YC, Osei-Hwedieh D, et al. Novel Targets of Drug Treatment for Pulmonary Hypertension. Am J Cardiovasc Drugs. 2015; 15(4): 225-34. Available from: https: //pubmed.ncbi.nlm.nih.gov/26016608/
- Roger I, Milara J, Montero P, Cortijo J. The role of JAK/STAT molecular pathway in vascular remodeling associated with pulmonary hypertension. Vol. 22, International Journal of Molecular Sciences. MDPI AG. 2021.
- Yerabolu D, Weiss A, Kojonazarov B, Boehm M, Schlueter BC, et al. Targeting Jak-Stat signaling in experimental pulmonary hypertension. Am J Respir Cell Mol Biol. 2021; 64(1).
- Miyawaki H, Kioka H, Sato K, Kurashige M, Ozawa T, et al. Longterm effects of the janus kinase 1/2 inhibitor ruxolitinib on pulmonary hypertension and the cardiac function in a patient with myelofibrosis. Internal Medicine. 2020; 59(2).
- Low AT, Howard L, Harrison C, Tulloh RMR. Pulmonary arterial hypertension exacerbated by ruxolitinib. Vol. 100, Haematologica. 2015.
- Tabarroki A, Lindner DJ, Visconte V, Zhang L, Rogers HJ, et al. Ruxolitinib leads to improvement of pulmonary hypertension in patients with myelofibrosis. Leukemia. 2014; 28(7).