
Open Journal of
Clinical and Medical Images
Short Report - Open Access, Volume 4
Scout marks the spot: A unique and novel use of wireless localization for retrieval and diagnosis of recurrence of Hodgkin lymphoma in the para-aortic lymph nodes
*Corresponding Author: Sydney A Caputo
Tulane School of Medicine, 1430 Tulane Ave, Box 8642,
New Orleans, LA 70112, USA.
Email: ascaputo@tulane.edu
Received : Jan 17, 2024
Accepted : Feb 14, 2024
Published : Feb 21, 2024
Archived : www.jclinmedimages.org
Copyright : © Caputo SA (2024).
Abstract
Although most patients with Hodgkin Lymphoma will achieve remission, those with advanced disease at diagnosis are at a risk of relapse of 15% to 30% [1,2]. Timing of recurrence of less than or equal to 12 months is one of the key risk factors used to evaluate patient prognosis and determine subsequent therapy [3-5]. Thus, accurate identification of relapse is of high importance so that patients may receive timely and adequate treatment for their disease.
Citation: Caputo SA. Scout marks the spot: A unique and novel use of wireless localization for retrieval and diagnosis of recurrence of Hodgkin lymphoma in the para-aortic lymph nodes. Open J Clin Med Images. 2024; 4(1): 1166.
Short report
We present a unique and novel approach for identifying lymph nodes for surgical resection with SAVI SCOUT (SCOUT) reflector in a patient with high suspicion for recurrent Hodgkin Lymphoma with FDG positive para-aortic lymph nodes although twice previously negative on core needle biopsy.
76 year-old female with a history of stage IV nodular sclerosis Hodgkin Lymphoma diagnosed May 2022 with extra nodal disease in L5, sternum, cervical lymph nodes and mediastinal lymph nodes status post 6 cycles A+AVD. Treatment was suspended after negative PET scan findings in November 2022.
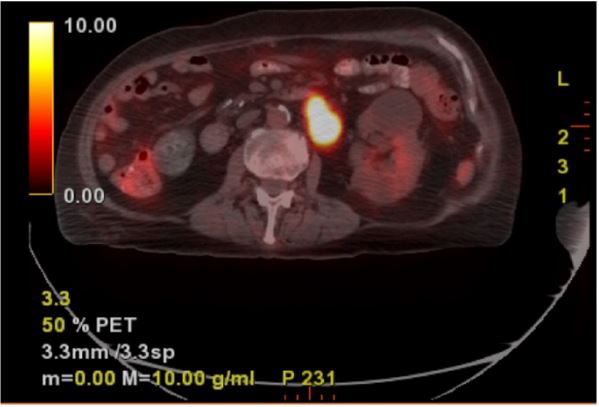
In January 2023 the patient was admitted for a GI bleed at which time EGD with biopsy revealed suspected B cell lymphoma. Computed Tomography (CT) scan of the neck in April 2023 showed heterogenous nodular density in thyroid bilaterally, intraspinal calcified mass T1 + T2 causing spinal stenosis. In June 2023 the patient’s FDG PET-CT fusion scan revealed a new left periaortic mass vs lymph node conglomerate measuring 2.8x4.2 cm with a Standardized Uptake Value (SUV) max of 19.7 (Figure 1). The scan also noted multiple new lesions with FDG avid activity ranging from SUV of 3.9-7.5 including a lymph node in the right lower neck adjacent to the thyroid gland, scattered mediastinal lymph nodes in the paratracheal region and AP window, and right hilar lymphadenopathy.
The patient subsequently underwent 2 CT-guided core needle biopsies in July 2023, both showing non-malignant, nonnecrotizing granulomatous inflammation. Although the needle biopsy results were both negative, there was still high concern for malignancy due to the patient’s history, high SUV of the PETCT, and recent EGD biopsy results of suspected B cell lymphoma.
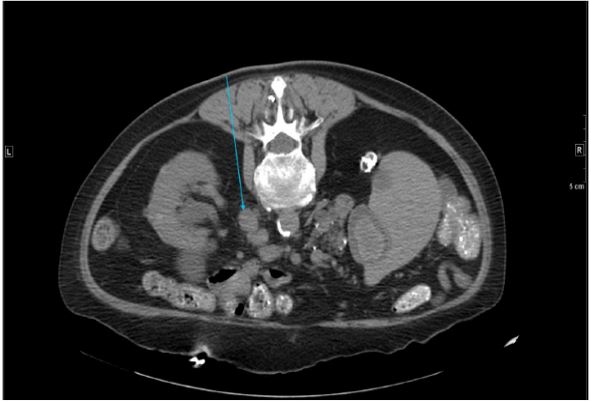
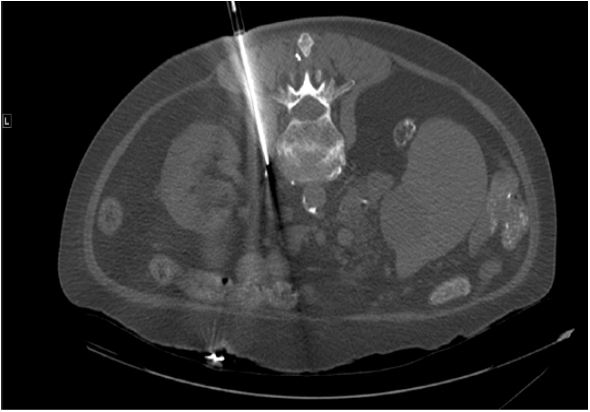
The patient was referred to surgical oncology for open biopsy of the lymph nodes. Plan for a SCOUT reflector was made to optimize retrieval of the actual PET avid node to increase both the sensitivity and specificity of the excisional biopsy. In addition, a reflector guided approach would minimize surgical exposure to potentially decrease post operative morbidity, decrease operative time, and enhance recovery in an elderly patient. The SCOUT reflector is an infrared activated, electromagnetic wavereflective implantable device [6]. CT-guided intra-abdominal SCOUT placement was performed via posterior approach adjacent to the left para-aortic mass measuring 3.0x1.4 cm (Figure 2A-C).
Reflector localized excisional biopsy of the left retroperitoneal lymph nodes was then performed via anterior transabdominal approach. The SCOUT signal was detected at the ligament of Treitz which was reflected and provided immediate exposure to the left retroperitoneal lymph node. Two lymph nodes were dissected and retrieved adjacent to the SCOUT reflector at the time of surgery. This was done through a 5 cm vertical midline supra-umbilical incision made over the area the SCOUT reflector was detected perioperatively. The patient had an uneventful recovery and was discharged home post-operative day 1. Flow cytometry of the left retroperitoneal lymph node failed to identify any abnormal cell populations. Hodgkin disease is classically associated with normal flow cytometry [7,8]. Final histopathology of the two retroperitoneal lymph nodes revealed classic Hodgkin Lymphoma.
Although typically used for patients with non-palpable breast cancer lesions as an alternative to wire localization, the expanded FDA approval for the SCOUT reflector in 2016 allows for placement of the device for localization of any soft tissue lesion. Used in breast cancer patients receiving Neoadjuvant chemotherapy to mark primary site as well as previously biopsied and clipped axillary nodes which may no longer be identified following response to Neoadjuvant chemotherapy [9]. Outside of breast cancer, it has also been used to identify areas for excision in a wide variety of patients such as those with non-palpable soft tissue sarcomas, melanoma metastasis and recurrence, leiomyosarcomas, malignant peripheral nerve sheath tumors, and pulmonary nodules [10-13]. The SCOUT Its use for a paraaortic lymph node excision biopsy is not described in the literature.
The utility of the SCOUT reflector in this patient is multifocal. The localization of the PET avid lymph nodes allows for a more directed and focused surgery. Thus, limiting the extent of midline incision to minimize morbidity of open approach and leading to a shorter surgery time and easier recovery without complications. Although core needle biopsy is a more minimally invasive approach to lymphoma diagnosis, it is often not as accurate as excisional lymph node biopsy and can lead to more instances of incorrect or nondefinitive conclusions [14]. With this patient, both core needle biopsies were negative for malignancy. Without lymph node excision and localization with the SCOUT reflector, it is very likely that this patient would have had delays in treatment which would have allowed for disease progression.

References
- Engert A, et al. Escalated-dose BEACOPP in the treatment of patients with advanced-stage Hodgkin’s lymphoma: 10 years of follow-up of the GHSG HD9 study. J Clin Oncol. 2009; 27(27): 4548-54.
- Eich HT, et al. Intensified chemotherapy and dose-reduced involved-field radiotherapy in patients with early unfavorable Hodgkin’s lymphoma: final analysis of the German Hodgkin Study Group HD11 trial. J Clin Oncol. 2010; 28(27): 4199-206.
- Brice P, et al. Analysis of prognostic factors after the first relapse of Hodgkin’s disease in 187 patients. Cancer. 1996; 78(6): 1293-9.
- Lohri A, et al. Outcome of treatment of first relapse of Hodgkin’s disease after primary chemotherapy: Identification of risk factors from the British Columbia experience 1970 to 1988. Blood. 1991. 77(10): 2292-8.
- Josting A, et al. New prognostic score based on treatment outcome of patients with relapsed Hodgkin’s lymphoma registered in the database of the German Hodgkin’s lymphoma study group. J Clin Oncol. 2002; 20(1): 221-30.
- Cox, C.E, et al. Pilot Study of a New Nonradioactive Surgical Guidance Technology for Locating Nonpalpable Breast Lesions. Ann Surg Oncol. 2016; 23(6): 1824-30.
- Beatriz Alvarez Flores M, et al. A new approach to the study of Hodgkin lymphoma by flow cytometry. Pathology. 2023; 55(1): 86-93.
- Morse EE, et al. The role of flow cytometry in the diagnosis of lymphoma: A critical analysis. Ann Clin Lab Sci. 1994; 24(1): 6-11.
- Lifrieri, A, et al. When the clipped node goes missing, CT guided SAVI SCOUT placement: A novel approach for localizing soft tissue targets. Clin Imaging. 2022; 85: 115-117.
- Broman, K.K, et al. Intraoperative Localization Using an Implanted Radar Reflector Facilitates Resection of Non-Palpable Trunk and Extremity Sarcoma. Ann Surg Oncol. 2021; 28(6): 3366-3374.
- Combs F, Y Maki. Inguinal Lymph Node Marked with SCOUT® Following Melanoma Surgery.
- Burke CJ, et al. Image-Guided Radar Reflector Localization for Small Soft-Tissue Lesions in the Musculoskeletal System. AJR Am J Roentgenol. 2023; 220(3): 399-406.
- Cornella KN, et al. A Surgeon’s Guide for Various Lung Nodule Localization Techniques and the Newest Technologies. Innovations (Phila). 2021; 16(1): 26-33.
- Syrykh C, et al. Lymph node excisions provide more precise lymphoma diagnoses than core biopsies: a French Lymphopath network survey. Blood. 2022; 140(24): 2573-2583.