
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Malignant insulinoma in dog: Case report
René Mandelík1 ; Marieta Ševčíková2 ; Viera Karaffová3 ; Viera Revajová3 ; Zuzana Ševčíková3*
1Department of Epizootology, University of Veterinary Medicine and Pharmacy in Košice, Parasitology and Protection of One Health, Komenského 73, 041 81 Košice, Slovak Republic.
2University Veterinary Hospital, Small Animal Clinic, University of Veterinary Medicine and Pharmacy in Košice, Komenského 73, 041 81 Košice, Slovak Republic.
3Department of Morphological Disciplines, University of Veterinary Medicine and Pharmacy in Košice, Komenského 73, 041 81 Košice, Slovak Republic.
*Corresponding Author: Zuzana Ševčíková
Department of Morphological Disciplines, University of
Veterinary Medicine and Pharmacy in Košice, Komenského 73, 041 81 Košice, Slovak Republic.
Email: zuzana.sevcikova@uvlf.sk
Received : Jan 25, 2024
Accepted : Feb 26, 2024
Published : Mar 04, 2024
Archived : www.jclinmedimages.org
Copyright : © Ševčíková Z (2024).
Abstract
In this case report, a malignant insulinoma is described in a thirteen-year old male dog of the Yorkshire breed. Clinical examination revealed weakness and food intolerance manifested by nausea and diarrhoea. Biochemically, hypoglycaemia with hyperinsulinemia, elevated concentrations of selected liver enzymes, as well as lipase and continuously increasing urea concentrations were also found. Ultrasonography of the pancreas proved the presence of a severe hypoechoic, homogenous lesion approximately 1 cm in diameter; the liver was diffusely heterogeneous with the occurrence of small hypoechogenic lesions in the parenchyma. With regard to history, clinical symptoms, USG and laboratory findings, insulinoma was diagnosed. Post-mortem findings showed a large, multifocal greywhite tumour in the right pancreatic lobe and enlargement of the liver, with the occurrence of many miliary foci. The corresponding lymph nodes of the pancreas and liver were also enlarged. Histopathological examinations of the pancreas and liver revealed malignant insulinoma.
Keywords: Dog; Insulinoma; Clinical and pathological findings.
Citation: Chen G, Wang Y, Liu Y, Li W. Pelvic radiation-induced sarcoma following treatment of cervical cancer. Open J Clin Med Images. 2024; 4(1): 1169.
Introduction
Pancreatic beta-cell tumours (islet cell adenoma-insulinoma and carcinoma-malignant insulinoma) are rare in humans and cats and uncommon in dogs. In humans, 90% of insulinomas are solitary and benign. In dogs, they are much more likely to be malignant, although morphological classification into adenoma or carcinoma does not consistently reflect the biological behaviour of these tumours. Metastatic lesions are detected in approximately 50% of canine insulinomas. They are seen most frequently from 5-12 years of age. Although many different breeds of dogs are affected, large breed dogs are overrepresented, while small breed dogs can also be affected, in particular west highland white terriers. Both sexes appear to be equally affected [1,2]. The insulinomas secrete excessive insulin because the negative feedback mechanism that is initiated by falling blood glucose levels is disrupted in the neoplastic β-cells. Therefore, the insulinomas cause profound hypoglycaemia [2].
Case presentation
A 13-year-old Yorkshire terrier male dog (5.8 kg) with general discomfort was presented. According to the owner, weakness and a food intolerance manifested by nausea and diarrhoea were observed in the last three months. Later, the owner described polydipsia and polyuria, as well. For the next eight months, samples of blood were taken 3 times from vena cephalica antebrachii for haematology and biochemistry examination.
Biochemical examinations showed hypoglycaemia (1.11 mmol/l, ref (reference range): 3.6-6.70 mmol/l) with hyperinsulinemia (136.6 mIU/l, ref: 9.00-32.00 mIU/l)) in the first sample. In the second and third samples normoglycaemia (4.77 mmol/l; 3.95 mmol/l) was detected. Elevated concentrations of selected liver enzymes (AST 0.81 µkat/l; 0.65 µkat/l, ref: 0.00-0.60 µkat/l, ALT 4.66 µkat/l; 3.54 µkat/l, ref: 0.00-0.95 µkat/l, and ALP 2.48 µkat/l; 16.08 µkat/l, ref: 0.00-1.24 µkat/l) and lipase (9.13 µkat/l, 24.84 µkat/l, ref: 0.00-5.00 µkat/l) as well, were registered in the first two samplings. Continuously increasing urea concentrations (8.48 mmol/; 10.99 mmol/l; 26.24 mmol/l, ref: 3.97-8.05 mmol/l) were also shown. The creatinine concentrations were in the reference ranges (49.8 µmol/l; 89.30 µmol/l, ref: 35.0-105.0 µmol/l).
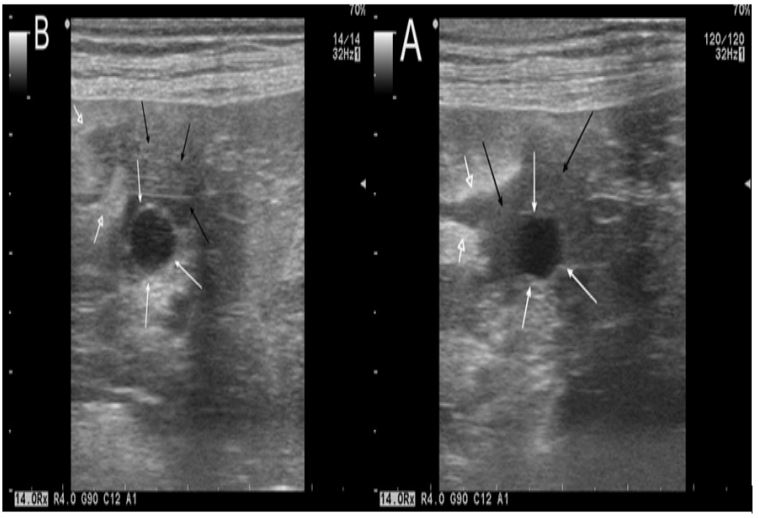
Ultrasound examination [Aloka Profound Alpha 6 ultrasonographic machine equipped with linear (5-16 MHz) and microconvex (5-10 MHz) probes] of the liver revealed diffuse heterogeneity, with the occurrence of small hypoechoic lesions in parenchyma (Figure 1A). In the pancreas the presence of severe hypoechoic, homogenous lesion approximately 1 cm in diameter and a reactive hyperechoic tissue consistent with acute pancreatitis were observed (Figure 1B).
With regard to history, clinical symptoms, USG and laboratory findings, insulinoma was diagnosed, and surgery was offered to the owner after informing her of the diagnosis. She rejected it due to the dog’s age and decided on euthanasia. Before euthanasia, the dog was sedated with medetomidine (Cepetor inj. 1 mg/ml inj., CP Pharma, Germany) and butorphanol (Butomidor 10 mg/ml inj., Richter Pharma AG, Austria), a combination of sedative and analgesic, which were administered intramuscularly. Subsequently, propofol at a dose 4 mg/kg b.w. was used intravenously for general anaesthesia. Euthanasia was performed intravenously using embutramide (T 61 inj., Intervet International B.V., Netherlands) at a dose 0.3 ml/ kg b.w. the owner agreed only with a partial necropsy.
During necropsy, a large grey-white tumour in the right pancreatic lobe and the enlargement of corresponding lymph nodes were found (Figure 2). In liver parenchyma many miliary foci of a whitish colour were observed scattered diffusely through the parenchyma. Hepatomegaly and enlargement of corresponding lymph node were observed.
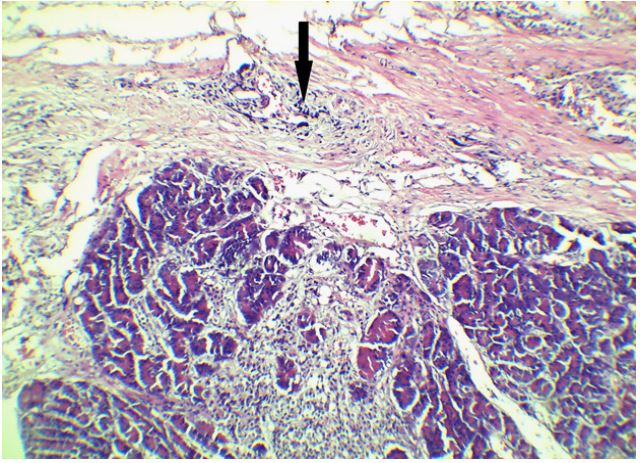
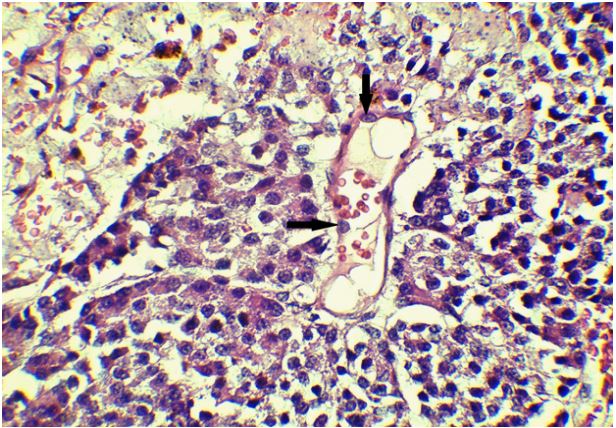
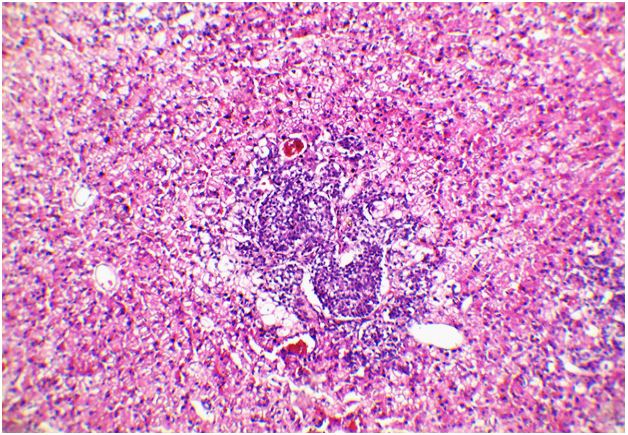
The tissue specimens for histology were taken from pancreas and liver. Large areas of neoplastic tissue were found in the pancreas. The invasion of neoplastic cells into the parenchyma (Figure 3A) and vessels (Figure 3B) as well, was seen. In the liver parenchyma islets of same cells were observed (Figure 3C).

Discussion
The most common pancreatic tumour in dogs is insulinoma [2]. However, it is also found in humans, cattle, cats and ferrets, in which the tumour is common, and are often associated with adrenal cortical tumours [3].
Clinical signs of insulinoma result from the effect of hypoglycaemia on the nervous system, which is termed neuroglycopenia. They may be present for days to months and are often intermittent or episodic [4]. In our case, there was only weakness and food intolerance manifested by nausea and diarrhoea. Later, polydipsia and polyuria were observed.
The diagnosis of insulinoma is confirmed by documenting hypoglycaemia (blood glucose <2.2 mml/l3 ) with a concurrent normal or elevated serum insulin concentration [1]. The values detected in this case corresponded with this scheme. Later, detected normoglycaemia was the consequence of long application of prednisolone in pill form (Prednicortone, tbl. 5 mg, LeLyPharma BV, Netherlands) at a dose of 0.5 mg/kg b.w.
A higher concentration of liver enzymes (AST, ALT and ALP) were found in the first two samplings. AST and ALT are enzymes contained in liver cells. When their levels are increased in the blood, it means that the enzymes have leaked out of the liver cells due to hepatocellular injury [5]. There are several forms of ALP elevation (nodular hyperplasia, blood vessel abnormalities and pancreatic neoplasia as well) but only in dogs is there a Corticosteroid - ALP (C-ALP), a form of ALP stimulated by the presence of steroids. So we assume that the elevation of liver enzymes in our case was caused by steroid medication at the same time as neoplastic liver and pancreas injury [6,7].
Moreover, the diagnosis of pancreatitis is hampered by the lack of a universally accepted gold standard, and no clinical signs or combination of them has been identified as pathognomonic for this disease in dogs [8]. Classically, elevations in serum amylase and lipase activity have been used as indicators of pancreatitis in dogs. On the other hand, they are not produced only in pancreas, so they can also be increased in nonpancreatic disease. Ex adverso dogs with confirmed pancreatitis may also have normal amylase and lipase activity [9]. We do not assume that the severe increasing of lipase activity in blood together with ultrasound finding of reactive hyperechoic tissue consistent with acute pancreatitis observed in our study represent sufficient data for confirmation of pancreatitis.
A higher concentration of urea was found throughout the whole case but the creatinine concentrations were in the reference ranges. Previously published cases of dogs with insulinoma reported different levels of urea [2,10,11]. In our case the course of disease did not point to renal and /or post renal insufficiency. We suppose that the higher urea levels were of prerenal origin caused by reduced renal perfusion. Creatinine can be influenced by muscle mass or breed of the dog, and its value can be decreased in a dog with cachexia or in a small breed dog [12], which fits with our case.
Malignant insulinomas can be macroscopically differentiated from islet cells adenomas by their large size, multi-lobular appearance, invasion into adjacent parenchyma and vessels and establishment of metastasis in extra pancreatic sites. Metastasis includes regional lymph nodes, liver, mesentery and omentum [3]. In this case, in addition to a large lesion localised in the right pancreatic lobe, miliary foci were found diffusely scattered throughout the liver parenchyma. They were evaluated as metastatic and confirmed by histological examination. The duodenal (right) lobe of the pancreas appears to be more frequently involved than the splenic (left) lobe [3], which complies with our work.
Conclusion
In summary the occurrence of malignant insulinoma in this case induced solid pancreatic tumour development with metastasis formations and some liver enzymes and urea elevation. It shows to the comprehensive negative impact of the tumour to the whole organism. Either specific therapy or surgery were rejected by owner.
Funding: None.
Conflict of interest: The authors declare no conflicts of interest.
References
- Lunn KL, Page RL. Pancreatic Beta-Cell Tumours (Insulinomas). In: Withthrow SJ, editor. Small Animals Clinical Oncology.5th ed. Elsevier. 2013; 519-531.
- Buishand FO. Current Trends in Diagnosis, Treatment and Prognosis of Canine Insulinoma. Vet Sci. 2022; 9 (10): 540. Available at: https://doi.org/10.3390/vetsci9100540
- Rosol TJ, Meuten DJ. Tumours of pancreatic islet cells. In: Meuten DJ, editor. Tumours in Domestic Animals, 5th ed. Wiley Blackwell. 2017; 822-828.
- Fukazawa K, Kayanuma H, Kanai E, et al. Insulinoma with basal ganglion involvement detected by magnetic resonance imaging in a dog. J Med Vet Sci. 2009; 71: 689-692.
- Ratnovsky M. What does it mean if a dog has elevated liver values. Available at: https://www.mspca.org/wp-content/uploads/2021/01/What-Does-it-Mean-if-a-Dog-has-Elevated-Liver-Values_Mara-Ratnofsky-DVM.pdf
- Alvarez L, Whittemore JC. Liver enzyme elevations in Dogs: Physiology and pathophysiology. Compendium: Continuing Education for Veterinarians. Available at: https://www.researchgate.net/publication/41549258_Liver_Enzyme_Elevations_in_Dogs_Diagnostic_Approach. 2009.
- Pettersson H, Ekstrand C, Hillström A, et al. Effect of 1mg/kg oral prednisolone on biochemical analytes in ten dogs: A cross-over study. Comparative Clinical Pathology. 2021; 30: 519-582.
- Cridge H, Twedt DC, Marolf AJ, et al. Advances in the diagnosis of acute pancreatitis in dogs. J Vet Intern Med. 2021; 35(6): 572- 587.
- Kenneth WS. Update on Pancreatitis in Dogs. In Proceedings: World Small Animal Veterinary Association Congress. 2006. https://www.vin.com/
- Kolevská J, Husník R, Brunclík V, et al. A Case of Canine Insulinoma. Acta Vet Brno. 2004; 73: 353-358.
- Jelínek F, Kuldová M, Vozková D, et al. Malignant insulinoma in Dog. [Maligní inzulinóm u psa. Kauzistické sdělení] Veterinární lékař. 2020; 8: 257-265.
- Misbach Ch, Chetboule V, Concordet D, et al. Basal plasma concentrations of routine variables and packed cell volume in clinically health adult small sized dogs: Effect of breed, body weight, age and gender, and establishment of reference intervals. Vet Clin Pathol. 2014; 3: 371-380.