
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Unveiling the uncommon: Lichenoid esophagitis secondary to Steven Johnson syndrome
Islam Mohamed*; Noor Hassan; Rawan Rajab; Manal Hassan; Lara Makhoul; Hassan Ghoz
McGee Trafficway, Kansas City, Missouri-64108, USA.
*Corresponding Author: Islam Mohamed
McGee Trafficway, Kansas City, Missouri-64108, USA.
Tel: 774-372-9318;
Email: Islamh3255@gmail.com
Received : Feb 05, 2024
Accepted : Mar 08, 2024
Published : Mar 15, 2024
Archived : www.jclinmedimages.org
Copyright : © Mohamed I (2024).
Abstract
Lichenoid Esophagitis (LE) is a rare pathology characterized by inflammation of the esophagus resembling a lichenoid pattern for which a precise histological diagnosis cannot be established. The diagnosis of LE is often challenging due to its nonspecific clinical presentation and lack of a definitive histological diagnosis. LE can cause various complications, including esophageal strictures, Barrett’s esophagus, dysphagia, esophageal ulcers, and an increased risk of esophageal cancer. Treatment options include proton pump inhibitors, dietary changes, and corticosteroids. In this report, we describe the case of a 47-year-old female who developed lichenoid esophagitis due to SJS as a result of sulfasalazine therapy.
Citation: Mohamed I, Hassan N, Rajab R, Hassan M, Makhoul L, et al. Unveiling the uncommon: Lichenoid esophagitis secondary to Steven Johnson syndrome. Open J Clin Med Images. 2024; 4(1): 1172.
Introduction
Lichenoid Esophagitis (LE) is a rare condition that has two main subtypes: Lichen Planus Esophagitis (LPE) and Lichenoid Esophagitis Pattern (LEP) [1]. While the exact cause of LE is unknown, it has been associated with factors such as lichen planus, viral infections, auto-immune disorders, and drug-induced reactions [2]. This report presents a case of a patient who developed LE following sulfasalazine therapy-induced Steven Johnson Syndrome (SJS). It highlights the potential association between SJS and LE and emphasizes the importance of considering LE in patients with dysphagia, particularly those with a history of drug-induced reactions or autoimmune disorders.
Case presentation
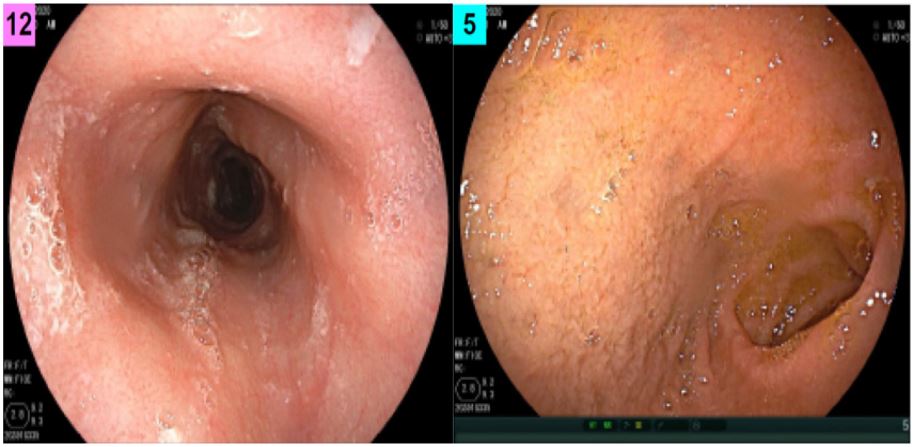
A 47-year-old woman with a medical history significant for Systemic Lupus Erythematosus (SLE) visited the Gastroenterology (GI) clinic for dysphagia. Her rheumatologist had referred her to GI after she complained of difficulty swallowing pills. An initial swallow evaluation showed moderate pharyngeal and esophageal dysphagia, and a flexible laryngoscopy was unremarkable. During her first upper Endoscopy (EGD), an esophageal ring was discovered (Figure 1). Pathology of biopsies revealed acute esophagitis with scattered fungal elements, and fluconazole was prescribed. Soon after, the patient followed up with her rheumatologist, and plans were made to start pharmacologic therapy for SLE. The patient was first given hydroxychloroquine, which resulted in a rash, and then methotrexate, which led to transaminitis. Ultimately, the patient was given Sulfasalazine (SSZ). Three weeks after starting SSZ, the patient urgently visited a care center due to lip swelling and throat tightness. SSZ was stopped and oral prednisone was given. Two days later, the patient was admitted to the emergency department with blistering of her lips and mucous membranes, as well as a painful macular erythematous blanching rash diffusely on her torso, limbs, palms, and soles, indicative of SJS. The patient had to be intubated and placed on mechanical ventilation due to acute hypoxemic respiratory failure but was later taken off the ventilator. Several months after recovery, the patient returned to the GI clinic, this time reporting worsening dysphagia and food regurgitation. EGD was performed and demonstrated a severe, benign-appearing intrinsic stenosis that was dilated (Figure 2). The patient was maintained on proton-pump inhibitor therapy and returned for repeat EGD 4 weeks later for re-dilation and biopsies. Biopsies were sent to an outside facility that confirmed lichenoid esophagitis. The patient has undergone 5 upper endoscopies with dilations following initial diagnosis. Despite being prescribed various H2 blockers and proton-pump inhibitors, the patient’s dysphagia showed minimal improvement. During the last two endoscopies, the patient received corticosteroid injections (triamcinolone) in addition to oral fluticasone and reported significant improvement in her symptoms.

Discussion
We present the first documented case in the literature of LE developing as a result of sulfasalazine-induced-SJS with subsequent esophageal stricture, contributing to the limited literature available on LE. Salaria et al was the first to classify LE into different categories, including LPE and LEP [1]. Histologically, LPE is characterized by atrophic epithelial cells, lymphocytic infiltrate, degenerated keratocytes (civatte bodies), and Direct Immunofluorescence (DIF) findings of IgM deposits at the dermo-epidermal junction and complement staining in apoptotic squamous cells [1]. Failure to meet both criteria leads to the classification of the condition as LEP.
Lichen Planus (LP) is a chronic, inflammatory skin condition that can also affect the mucous membranes and nails [3]. The cause of LP is not well understood, but it is thought to be related to an autoimmune reaction, viral infection, or medication reaction [1]. LP can manifest in different forms, including as small, itchy, purple papules or plaques on the skin or mucous membranes [4]. In some cases, LPE may occur before the appearance of skin lesions, which are the classic hallmark of LP [5]. This is known as “isolated LPE” or “primary LPE.” In other cases, LPE may occur concurrently with skin lesions, known as “secondary LPE” [5]. LP is generally considered a rare disease, with estimated incidence rates of 0.4% in the USA [6]. The condition is more common in middle-aged adults and affects both men and women equally. LE is even more rare with reported estimated incidence of 0.03% [7]. A careful review of the patient’s medical history and physical examination failed to reveal any evidence of LP affecting the skin or mucous membranes.
According to Salaria et al. patient-related factors such as rheumatological disorders, polypharmacy, and viral infections were found to be associated with an increased incidence of LE [1]. The study revealed that 59% of LEP patients used more than three medications, 11% had a rheumatological disease, and 9% had a diagnosis of viral hepatitis, while 14% had HIV [1]. Our patient’s prescription list exceeded three medications, and this, when combined with the patient’s history of SLE, increases their likelihood of experiencing LEP.
Although LE is a rare condition, it is important to recognize because it can lead to significant morbidity and decreased quality of life. There is currently limited data on the association between LE and malignancy. However, a few case reports have suggested a possible link between LE and squamous cell carcinoma of the esophagus [8].
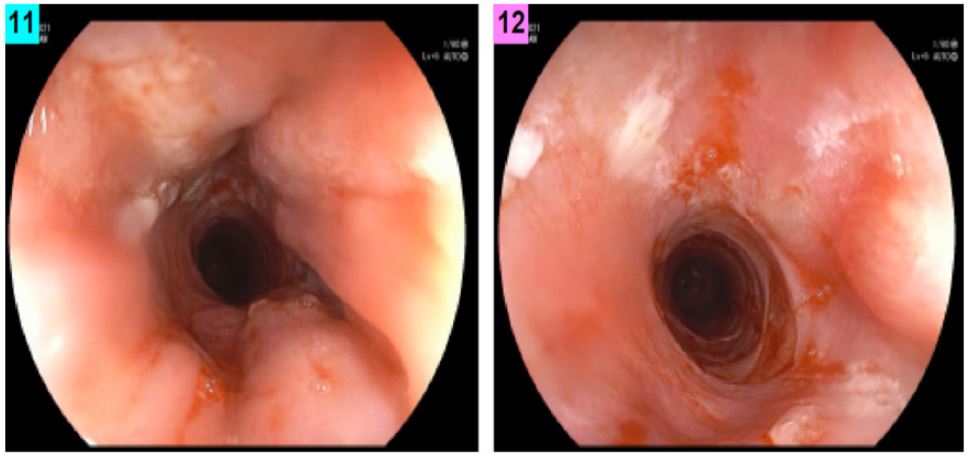
Unlike oral and cutaneous lichen planus manifestations, there are currently no therapeutic guidelines for esophageal lichen planus. However, the use of intralesional steroid injections has been studied as a treatment of lichen planus-associated esophageal stenosis in several case reports and case series. Early studies tested triamcinolone injections without the use of any adjunctive therapies, which provided symptomatic relief for up to six months prior to the recurrence of symptoms necessitating repeat treatments [9-11]. Alternatively, it appears that intralesional triamcinolone produced the best results when used in combination with esophageal balloon dilation and a 7-day course of oral steroids before and after the procedure, with an average interval of eight months between symptom recurrence [12]. Additionally, due to the increased incidence of superficial esophageal mucosal tearing, endoscopists preferred to administer the intralesional steroids prior to the balloon dilatation. Addressing mechanical obstruction while simultaneously treating the local inflammatory lesion seems to be the most effective strategy to alleviate common symptoms such as dysphagia or odynophagia. In our patient’s case, multiple dilatations were required due to refractory symptoms despite the use of PPIs and H2 blockers. However, after we attempted corticosteroid injection and swallowed fluticasone the patient eventually experienced an improvement in their symptoms and endoscopic findings (Figure 3).
Due to the lack of previous reports of LE secondary to SJS or sulfasalazine, the case presented in this report is of particular interest. It highlights the importance of considering it in the differential diagnosis of dysphagia in patients with a history of drug-induced reactions. Further research is needed to better understand the pathogenesis and optimal treatment of this rare condition. Our experience highlights that intralesional steroids in addition to topical steroids can be effective for relief of dysphagia symptoms in Lichenoid esophagitis.
Declarations
Acknowledgment statement: We extend our appreciation to all individuals who contributed to the completion of this study.
Funding information: This research was conducted without specific external funding.
Conflict of interest statement: The authors affirm that there are no conflicts of interest related to this study.
References
- Salaria SN, Abu Alfa AK, Cruise MW, Wood LD, Montgomery EA. Lichenoid esophagitis: Clinicopathologic overlap with established esophageal lichen planus. Am J Surg Pathol. 2013; 37(12): 1889-94. doi: 10.1097/PAS.0b013e31829dff19.
- Shergill, Annie MD. S2401 A Rare Case of Lichenoid Esophagitis Causing Refractory GERD. The American Journal of Gastroenterology. 2022; 117(10S): e1606. DOI: 10.14309/01.ajg.0000866244.36964.63
- Gorouhi F, Davari P, Fazel N. Cutaneous and mucosal lichen planus: a comprehensive review of clinical subtypes, risk factors, diagnosis, and prognosis. ScientificWorldJournal. 2014; 2014: 742826. doi: 10.1155/2014/742826.
- Katta R. Lichen planus. Am FAM Physician. 2000; 61(11): 3319-24, 3327-8. Erratum in: Am Fam Physician 2000 Oct 15; 62(8): 1786.
- Katzka DA, Smyrk TC, Bruce AJ, Romero Y, Alexander JA, et al. Variations in presentations of esophageal involvement in lichen planus. Clin Gastroenterol Hepatol. 2010; 8(9): 777-82. doi: 10.1016/j.cgh.2010.04.024.
- Leasure AC, Cohen JM. Prevalence of lichen planus in the United States: A cross-sectional study of the All of Us research program. J Am Acad Dermatol. 2022; 87(3): 686-687. doi: 10.1016/j.jaad.2021.12.013.
- Haque, Salima MD; Shore, Keddy; Turner, Kevin O. DO; Genta, Robert M. MD, FACG. S407 Lichenoid Esophagitis: A Clinical Entity with Distinct Manifestations. The American Journal of Gastroenterology. 2021; 116: S180. DOI: 10.14309/01.ajg.0000774100.93487.fa
- Thomas M, Makey IA, Francis DL, Wolfsen HC, Bowers SP. Squamous Cell Carcinoma in Lichen Planus of the Esophagus. Ann Thorac Surg. 2020; 109(2): e83-e85. doi: 10.1016/j.athoracsur.2019.05.062.
- Franco DL, Islam SR, Lam-Himlin DM, Fleischer DE, Pasha SF. Presentation, Diagnosis, and Management of Esophageal Lichen Planus: A Series of Six Cases. Case Rep Gastroenterol. 2015; 9(2): 253-60. doi: 10.1159/000437292.
- Reissmann A, Hahn EG, Faller G, Herold C, Schwab D. Sole treatment of lichen planus-associated esophageal stenosis with injection of corticosteroids. Gastrointest Endosc. 2006; 63(1): 168-169. doi:10.1016/j.gie.2005.07.045
- Rao B, Gulati A, Jobe B, Thakkar S. Esophageal Lichen Planus: Understanding a Potentially Severe Stricturing Disease. Case Rep Gastrointest Med. 2017; 2017: 5480562. doi: 10.1155/2017/5480562.
- Wedgeworth EK, Vlavianos P, Groves CJ, Neill S, Westaby D. Management of Symptomatic Esophageal Involvement with Lichen Planus. Journal of Clinical Gastroenterology. 2009; 43(10): 915-919. doi: 10.1097/MCG.0b013e31819db2df.