
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Point-of-care ultrasound in necrotizing pneumonia: A case report in an adult
Heesun Choi1*; Aurelia C Kucera1; Phillip Hasenbalg2
1Department of Emergency Medicine, Kingman Regional Medical Center, 3269 Stockton Hill Rd, Kingman, AZ 86409, USA.
2Department of Emergency Medicine, University of California Irvine, Orange, CA, USA.
*Corresponding Author: Heesun Choi
Department of Emergency Medicine, Kingman Regional
Medical Center 3269 Stockton Hill Rd Kingman AZ 86409, USA.
Tel: 949-233-7086;
Email: heesunchoido@gmail.com
Received : Feb 17, 2024
Accepted : Mar 12, 2024
Published : Mar 19, 2024
Archived : www.jclinmedimages.org
Copyright : © Choi H (2024).
Abstract
Case presentation: A 49-year-old woman returned to the emergency department for respiratory distress and pleuritic chest pain one day after influenza diagnosis. Chest X-ray was consistent with pneumonia. Point-of-care ultrasound showed dynamic air bronchograms and computed tomography revealed necrotizing pneumonia.
Discussion: Emergency physicians should suspect necrotizing pneumonia in patients with rapidly progressive community-acquired pneumonia. Point-of-care ultrasound can aid in quick diagnosis of pneumonia. Emergency physicians should be familiar with ultrasound and computed tomography findings in necrotizing pneumonia to trigger appropriate treatment.
Keywords: Necrotizing pneumonia; Point-of-care ultrasound; Dynamic air broncho grams; Case report.
Citation: Choi H, Kucera AC, Hasenbalg P. Point-of-care ultrasound in necrotizing pneumonia: A case report in an adult. Open J Clin Med Images. 2024; 4(1): 1173.
Case presentation
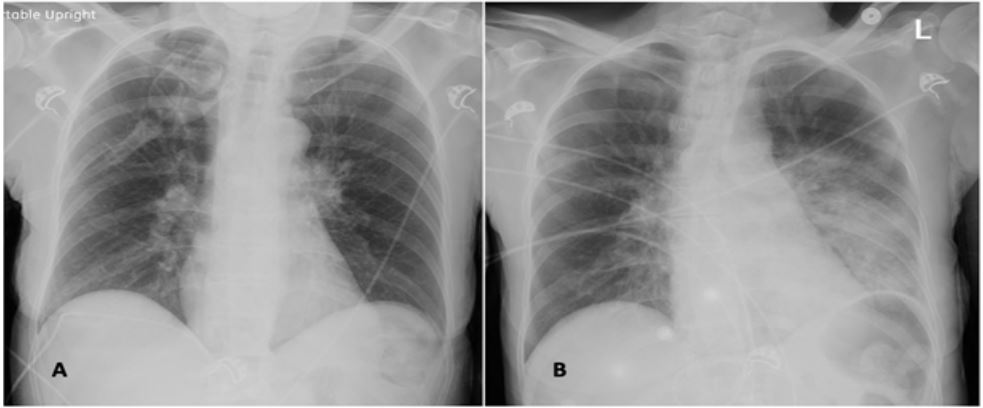
A 49-year-old woman with a history of anxiety, tobacco, and methamphetamine use, presented to the Emergency Department (ED) for one week of cough and body aches. She had normal vital signs and Chest X-Ray (CXR) showed no evidence of acute pathology (Figure 1). She was discharged home after positive influenza a testing. Twenty hours later, the patient re-presented to the ED for respiratory distress and new-onset pleuritic chest pain. She was tachycardic, hypotensive, febrile, and hypoxemic. Repeat CXR showed dense opacities in the left lung (Figure 1). A central line was placed and vasopressors and intravenous (IV) antibiotics were started. She was admitted to the intensive care unit for Community-Acquired Pneumonia (CAP), acute respiratory failure, and septic shock. Non-invasive ventilation was used initially, but she required intubation within several hours.
Emergency medicine residents performed Rapid Ultrasound for Shock and Hypertension protocol at bedside and found dense consolidations in the left lung with dynamic air bronchograms and a small pleural effusion (Figure 2). Computed Tomography (CT) revealed necrotizing pneumonia (Figure 3). The patient then developed a left-sided pneumothorax; a chest tube was placed with near-resolution of the pneumothorax. Blood and sputum cultures revealed methicillin-resistant Staphylococcus aureus and the patient was continued on appropriate IV antibiotics.


Discussion
Necrotizing pneumonia is an uncommon complication of CAP, affecting fewer than 1% of adult CAP cases and up to 7% of pediatric cases [1,2]. The disease progresses rapidly, even in otherwise healthy young adults, and patients often present in severe sepsis [1]. Risk factors for development of necrotizing pneumonia include influenza co-infection, tobacco use, heavy alcohol use, drug abuse, and gastrectomy [1].
The most common causes of necrotizing pneumonia are S. aureus, Streptococcus pneumoniae, and Klebsiella pneumoniae [1]. Both methicillin-resistant and methicillin-sensitive strains of S. aureus can express Panton-Valentine Leucocidin (PVL), an exotoxin that causes cell death; PVL-positive S. aureus is associated with severe necrotizing pneumonia and reduced survival [1]. Necrotizing pneumonia is difficult to treat and may require surgical intervention, particularly when it progresses to pulmonary gangrene or bronchopulmonary fistula [1].
Diagnosis of necrotizing pneumonia relies on imaging. CT is standard in adults as CXR rarely shows evidence of lung necrosis, and necrotizing pneumonia can be diagnosed by ultrasound in pediatric patients [1,2]. CT findings include lung consolidation, loss of normal parenchymal structure, loss of parenchymal enhancement (tissue liquefaction), and pneumatoceles or abscesses [1,2]. Ultrasound findings of pneumonia include multiple B-lines, pleural effusion, sonographic consolidation or hepatization, and dynamic air bronchograms [3,4]. In dynamic air bronchograms, air reflections move with respiration, distinguishing pneumonia from atelectasis [4]. Ultrasound in pediatric necrotizing pneumonia often shows consolidation with hypoechoic lesions (pneumatoceles) and pleural effusion [2]. Detection of pneumatoceles was influenced by depth of the necrotic tissue [2]; pneumatoceles may therefore be more difficult to detect in adults, particularly obese or severely ill patients, due to position.
Emergency physicians should consider necrotizing pneumonia, particularly in children and healthy adults with rapidly progressive illness. Point-of-care ultrasound is useful in diagnosing pneumonia and can be followed by CT in adults for early recognition of necrotizing pneumonia to trigger appropriate care.
Disclosure: Authors have no current of past relationship with commercial entities.
References
- Krutikov M, Rahman A, Tiberi S. Necrotizing pneumonia (aetiology, clinical features and management). Curr Opin Pulm Med. 2019; 25: 225-232.
- Carrard J, Bacher S, Rochat-Guignard I, et al. Necrotizing pneumonia in children: Chest computed tomography vs. lung ultrasound. Front Pediatr. 2022; 10: 898402.
- Kameda T, Mizuma Y, Taniguchi H, et al. Point-of-care lung ultrasound for the assessment of pneumonia: A narrative review in the COVID-19 era. J Med Ultrason. 2021; 48: 31-43.
- Lichtenstein D, Mezière G, Seitz J. The dynamic air bronchogram. A lung ultrasound sign of alveolar consolidation ruling out atelectasis. Chest. 2009; 135(6): 1421-1425