
Open Journal of
Clinical and Medical Images
Research Article - Open Access, Volume 4
Implementation of remote MRI scanning
Clay Hinrichs*; Seela Hinrichs; Ryan Scholte
Touro College of Osteopathic Medicine, New York, USA.
*Corresponding Author: Clay Hinrichs
Adjunct Clinical Assistant Professor, Touro College of Osteopathic Medicine, New York, USA.
Assistant Professor of Diagnostic Radiology Rutgers New
Jersey Medical School, USA.
Tel: 732-713-4299;
Email: chinrichsmd@imagecarecenters.com
Received : Apr 05, 2024
Accepted : Apr 24, 2024
Published : Apr 30, 2024
Archived : www.jclinmedimages.org
Copyright : © Hinrichs C (2024).
Abstract
The present shortage of MRI technologists continues to interfere with the delivery of care of patients. In addition, there have been limited solutions to cover disability, sickness, vacation, and personal days of that limited workforce. Our practice decided that the best way to address these coverage problems was to implement a virtual remote scanning solution. We explain the IT infrastructure, training and policies needed to implement this innovative solution safely and successfully to the MRI technologist shortage.
Introduction: The present shortage of MRI technologists continues to interfere with the delivery of care of patients. In addition, there have been limited solutions to cover disability, sickness, vacation, and personal days of that limited workforce.
Methods: Our practice decided that the best way to address these coverage problems was to implement a virtual remote scanning solution.
Results: We explain the IT infrastructure, training and policies needed to implement this innovative solution safely and successfully to the MRI technologist shortage.
Conclusion: Virtual remote scanning can be a safe and effective solution to address MRI technologist shortage.
Implications for practice: Virtual remote scanning can be a safe and effective solution to address MRI technologist shortage.
Citation: Hinrichs C, Hinrichs S, Scholte R. Implementation of remote MRI scanning. Open J Clin Med Images. 2024; 4(1): 1181.
Introduction
The current shortage of MRI technologists has impacted imaging coverage in most hospital and outpatient practices [1-3]. The field of radiology battles a never-ending leakage of qualified technologist coverage as a result of disability, sickness, vacation, and personal days. The loss of technologists to higher wages and competing health systems is also a significant problem. Per diem technologists who are willing to pick up shifts on short notice are extremely rare. Locums’ coverage requires advance planning and typically is extremely expensive. Overtime is always an option, but this further erodes the limited margins in managing an imaging practice. The pressure of splitting the outpatient dollar continues to be problematic and, in most cases, the above-described options are unlikely to provide a solution to anyone but the largest institutions with significant endowments. Furthermore, the pool of candidates who are properly qualified to perform highly specialized scans such as cardiac MRIs is extremely small. Recruiting and retaining this highly trained subset of individuals is difficult at best, and virtually impossible at every location.
Unfortunately, many of the above-described solutions have been unsuccessful for most practices, including ours. Most outpatient practices in such situations scramble to find last-minute and long-term imaging coverage. When we are unable to do so, which happens frequently, we need to cancel appointments and reschedule patients, which further burdens our front desk and call centers. The difficulty of rescheduling specialized MRIs is even greater because they can only be performed at a limited number of facilities by highly specialized technologists, for whom replacements cannot be easily found. As a direct result of this rescheduling uncertainty, patients’ satisfaction declines and their confidence in their healthcare providers erodes.
The outlook for hospital and health systems is even bleaker because they need to provide 24/7 coverage, which poses a bigger challenge than providing coverage during normal business hours. This leads to many health systems requiring back-up call to cover callouts which come at a cost, both financially and with staff retention. These call burdens further weaken staff recruitment and retention. Some hospital systems are forced to mandate overtime in certain circumstances to provide much needed coverage, which is not ideal for many reasons but especially when it comes to patient safety.
Although our practice is in a suburban area, we have continued to struggle with ensuring adequate technologist coverage at our facilities. An additional challenge faced by our practice is the vast geographical area we cover; we have twenty MRIs which are spread throughout the North, West and Central New Jersey regions, therefore moving technologists laterally across the system is nearly impossible. Most of our technologist’s object to regularly moving amongst multiple facilities, which is understandable because some may not have familiarity with the equipment or workflow in the other imaging centers. Employee satisfaction is always a consideration given the continued competition of nearby facilities when requiring cross-coverage.
Our practice decided that the best way to address these coverage problems was to implement a virtual remote scanning solution throughout our centers through the use of Siemens’ Syngo Virtual Cockpit (SVC) [4]. The primary goal was to strategically roll out SVC in all of our MRI facilities, which required a multipronged approach. First, we needed to test and partially upgrade our IT infrastructure to support this objective. Second, we needed to develop policies and procedures for the safety of our patients and staff. Third, we had to develop a training and safety program for our technologists and technologist assistants. Lastly, we also needed to appreciate that incorporating SVC would require us to reassess our workflow and front desk coverage.
Our secondary goal was to implement Siemens’ We-Scan [5] across our organization to enable virtual coverage for imaging services. Through We-Scan, Siemens offered the services of licensed MRI technologists to virtually cover our facilities for six days a week, and up to three scanners at a time.
IT infrastructure and testing
Under our original setup, our twenty MRIs utilized a mixture of business level cable modems and fiber. We also had a small MPLS (multiprotocol label switching) network covering two magnets and were in the process of upgrading our entire network to ELAN (Ethernet Local-Area Network) and eliminating the MPLS. During our initial testing and validation, we quickly realized that using cable modems caused large latency and jitter between both the SVC server and their respective steering stations. We also discovered that cable modems, even ones designed for commercial use, utilize a shared medium which equates to over subscription of the service provider during peak hours. Siemens requires a strict 25 millisecond latency threshold which will manifest as poor performance if that threshold is not met. In order to mitigate this issue, we opted to deploy dedicated fiber transports or utilize low latency queuing on egress interfaces within the network.
Such infrastructure enabled the system to bypass internet service policies and carrier congestion, which is traditionally considered best effort outside of the WAN (Wide-Area Network) edge. Utilizing private WAN links enabled us to have full control of bandwidth across all locations while giving us the flexibility to consider failover and load balancing techniques. ELAN terminating devices were used to route local traffic to all branch offices while seamlessly allowing networks to span the remote edge utilizing carrier Ethernet techniques.
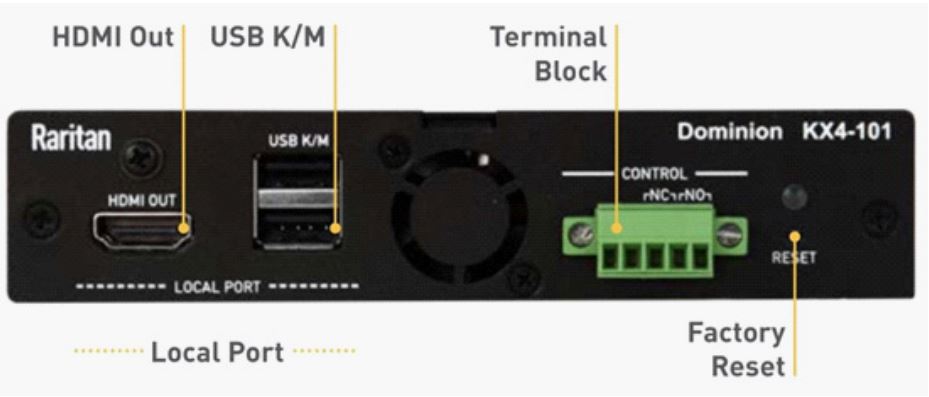
We have deployed SVC across all our Siemens and non-Siemens MRIs. The Siemens platforms which had access to Syngo Expert-I (Expert-I) to connect with SVC used that connection method. Expert-I allows interactive remote assistance during the MRI exam and provides real-time access to imaging data and exam information from any networked PC within the network. The non-Siemens units and the Siemens MRI without access to Expert-I required a KVM (Keyboard, Video, and Mouse) switch (Figure 1). A KVM switch is a device which connects a keyboard, monitor, and mouse to multiple computers and allows control and switching between them. It has the ability, depending on the model, to access other connections such as audio and USB ports. Local network infrastructure may also require a KVM switch on a Siemens platform with access to Expert-I. This issue will be discussed in greater detail below.
As mentioned above, because latency drives everything in SVC, a robust network and dedicated individuals willing to deploy QOS (Quality of Service) are a necessity for success. QOS is the concept of prioritizing traffic by treating varying classes of traffic differently. Our resident network engineer took a holistic approach by spending time understanding individual traffic flows and business requirements. Traffic that needs priority, such as SVC, must be considered front and center if a successful rollout is desired. Radiology networks are notorious for the sheer volume of data that travels through a given network during a sampled time period; therefore, congestion in network links is always a concern and must be addressed. Devices which support multiple QOS queues and thresholds are recommended, if not required, as it allows for a more granular traffic association as many processes may have various different levels of priority.
In our organization, we run VoIP (Voice over the Internet Protocol), which is a priority, on our QOS as we do not want to drop voice packets or have call degradation as a result of SVC implementation. In addition, bandwidth competition is always a concern when sending massive tomosynthesis studies as they interfere with our latency and therefore our ability to connect to the MRI with SVC. Having the voice phone traffic classified, marked and queued in a low latency queue is of utmost importance, followed by a priority queue matching SVC traffic patterns. Real time traffic sensitive to latency such as SVC should be prioritized directly after voice. This classification ensures that if congestion hits the egress interface facing the WAN edge, it has dedicated bandwidth and scheduling time by the network device to function properly. Be mindful that allocating too much buffer space in QOS could result in higher latency as data is buffered for a period of time that may exceed the Expert-I and KVM latency threshold. We found this phenomenon, commonly known as buffer bloat, to most often occur with Expert-I. If you are unable to deploy this successfully, then KVM switches across the system are the way to go as they require far less bandwidth. However, be aware that there is a higher cost associated with procuring the supported KVM switches as many, if not most, are purchased by the military for non-commercial purposes and you will pay a premium for them.
As for metrics, our network engineer measured sample SVC traffic across the following three controls: (a) Expert-I native connection; (b) Expert-I over https (newer software); and (c) KVM switch. During peak stress, the output was as follows: 65 mbps, 98 mbps and 22 mbps, respectively. The greater the output, the more stress there was on downstream equipment which, in turn, resulted in bottlenecks impacting SVC latency. As the numbers reflect, KVM is the top performer from a bandwidth output perspective.
If you use Expert-I communication channels to connect to modalities using SVC, keep the following considerations in mind. One of our biggest delays rolling out the product was the limited information that we were able to obtain regarding the ports, protocols, and services utilized by Siemens to connect from SVC to the MRI itself. Within the SVC infrastructure configuration manager, there are several options to choose from for your transport method. There are three Expert-I settings and one KVM option (which we will not cover here). Our delay during initial testing was caused by not understanding which Expert-I connection method to use on a per-MRI basis as well as which port to connect to. After several attempts, our network engineer had to run packet-captures within the network to finally understand the connection settings. Consider having someone who is proficient at network troubleshooting involved in this process as it can be a major hurdle in implementation.
If utilizing KVMs, there are some unique considerations which must be considered prior to implementation. This device is simple to connect. The AWS (MRI acquisition workstation) video is connected to the KVM via a video cable. The input on the KVM is an HDMI (High-Definition Multimedia Interface). The output from the AWS varies but is most often a DVI connector. A USB-to-USB cable is also used to connect between the AWS and KVM and the mouse and keyboard is disconnected from the AWS and plugged directly into the KVM. The native ethernet cable connected into the AWS remains, and an additional ethernet is connected into the KVM. A full understanding of the KVM workflow and data exchange process was something that our IT staff needed to grasp as it is an integral part of understanding how the system works from an IT supportability perspective. Someone familiar with SSL (Secure Sockets Layer) certificates and certificate authorities should be involved on any deployment as connections to and from the KVM must be validated via SSL certificates not only on the SVC server infrastructure, but also every steering and modality client workstation. Sites with domain controllers would benefit from their internal DNS (Domain Name System) servers be registering KVMs to their local DNS databases for easy look ups. In our case, some more thought had to go into this topic as we utilize three different domains. For instance, we leveraged host files within the Windows operating system to resolve hostnames to correct IP (Internet Protocol) addresses that also needed to match certificate names and SANS (SysAdmin, Audit, Network, and Security). This is used to validate that the application is correctly receiving secure data from the correct KVM.
After overcoming the initial hurdle of getting secure IP connectivity to the KVM switches, it is important to follow the SVC installation manual closely as the application is extremely strict for data verification. Within the SVC server manager, there is a technical configuration page where you must enter the appropriate data per KVM and per license, which is known as the “modality configuration.” One field within the modality configuration page consists of entering in the FQDN (Fully Qualified Domain Name) of the modality client. During initial set up, IT struggled with trying to allow modality clients to generate “on the fly” KVM credentials for? the SVC steering technologist using Siemens configured backend APIs (Application Programming Interface) to the KVM switches. The FQDN within this page required the full name of the host workstation, identified as the modality client workstation, to be entered in and the data must be case sensitive.
Steering clients (technologist controlling workstations) connecting to KVMs must also be configured correctly to allow proper communication to and from both devices. The steering client workstation required additional software to allow the SVC software to make the KVM data feed appear correctly on the SVC application. The first challenge we encountered was understanding that not only did the SVC infrastructure need the KVM certificate stored in the Windows trust store, but also on the steering workstation. The logic from the application design is to have the steering client submit a connection to the KVM in which the server sends a direct request to generate credentials. The SVC infrastructure server then communicates with the KVM using the modality configuration settings and SSL certificates loaded into the trust store to negotiate a secure encrypted channel. From there, the specified KVM generates an “on the fly” modality login for the steering technologist to authenticate the KVM itself. When the steering client ultimately uses the credentials to log-in, the steering client then connects directly to the KVM using the same method as the SVC infrastructure server.
Once a secure channel from both the SVC server and the steering client is established and authenticated, the last step is for the application to understand how to handle that data stream. This is where a third-party tool kit, which in our case was AKC (active kvm client), is utilized. The AKC client is software from the KVM manufacturer that allows third parties to interface with applications. SVC needs a mechanism to transfer data from the KVM, which is not compatible with Siemens, to SVC; AKC client is the mechanism that allows SVC and KVM to interface. Without AKC client, when you launch SVC through a KVM, the system freezes. AKC client allows the proper display of the KVM vendor’s software into the SVC software. It is important to understand that the AKC client tool kit must be deployed in the correct SVC file path to enable the KVM data feed to be displayed correctly within the SVC application itself.
Once a secure channel is established and the data is displayed within the SVC client application, IT initially had problems obtaining the correct resolution to display from the Modality Acquisition Workstation (AWS) onto the steering client monitors. This is due to the KVM acting as the negotiator trying to link native resolutions across two substantially different, and possibly unsupported, devices (i.e., AWS and a native steering station 4k monitor). Our IT staff had to spend some time customizing resolutions until a successful and reliable process was devised.
SVC utilizes and depends on reliable camera feed positioned down the bore of the MRI, as well directly at the contrast injector. During the initial camera set up, IT staff spent time obtaining the most optimal settings to yield a real-time camera experience. In all instances, the resolution, frame rate, bitrate and image saturation across all locations remained identical and resulted in a favorable outcome. It is important to understand that with Real Time Streaming Protocol (RTSP) cameras, there will be inherent delays with receiving the data on screen despite the protocol’s name. This delay is mostly caused by the receiving end having to decode the information which can be processor intensive. Although SVC technicians were initially under the impression that zero delay was achievable, after many attempts of technical measures, the average delay time stood at about one second.
SVC utilizing RTSP cameras with high compression codecs should also be a consideration during the design phase. A high compression codec susceptible to network congestion can cause extreme loss of real time video if packets are dropped. This is because if one compressed packet is lost, the remote viewer will lose the equivalent of uncompressed data in terms of frames, which will result in a substandard experience.
Given our original infrastructure, SVC was set up in a way where each MRI location had the ability to run any magnet in our system, which required a dedicated VPN from each site to every other site. As you can imagine, for an organization with over twenty facilities, we have a tremendous number of VPN connections across the system. When we eventually deploy ELAN, these will no longer be needed as data will be routed to a remote location over the private circuits. However, these firewall VPNs will ultimately be available in the event a local site loses its connection to the private WAN and a backup VPN needs to be utilized. This design consideration was the reason we opted not to wait for ELAN deployment to go live.
We rolled out SVC at one location per week over a period of time, testing and re-testing the system in all directions. IT staff and our lead technologist were heavily involved during this period validating all successful communications and performance complaints. To expedite troubleshooting of both clinical and performance issues, it is important to pair IT staff with a technically savvy MRI technologist who can “translate” and be a liaison between the clinical and IT staff.
One of the first challenges we encountered was that the SVC workstations (Figure 2) which were utilizing SVC were underpowered. Although our initial workstation devices were from the recommended Siemens specifications, we quickly noted that while using SVC, the CPU of the steering station was being highly utilized in the 90 percentile while trying to stream and process SVC traffic across the network. IT discovered that most, if not all, of the SVC MRI graphical data was being processed by the CPU, and little to none by the actual graphical processing unit. This caused the workstations to require additional CPU resources, a shortcoming we did not anticipate. Our first trial workstation was an 8 core Intel I5 processor, but given the problems we encountered, we moved to a 12 core Intel I7 to address CPU overutilization. When considering the SVC workstation selection, we recommend overprovisioning the workstation as opposed to under provision, especially if the anticipated workstation will be steering multiple MRIs. Our final standard deployable workstation was determined to be an Intel Core I7, 12TH generation or newer, paired with 16 GB of DDR5 memory, as well as a M.2 NVME SSD for disk, paired with two 4k monitors, which are scalable to 2560 x 1440.
When selecting monitors, you should purchase monitors with 4k resolution as per Siemens specifications. When the IT staff was finally ready to test the application with MRI technologists, we quickly realized that the native 4k resolution paired with SVC did not work well together. We concluded that what yielded the best experience from the MRI technologist’s perspective was to use 2560 x 1440 resolution, while also having no scaling enabled on the workstation. In addition, with this setting, the application did not throw any ambiguous errors at the actual user trying to steer a remote modality.
Utilizing voice and audio through the application is straightforward and leverages the built-in tool provided by Siemens. Once an auxiliary device is plugged into the physical workstation, Siemens lets you select the input and output device to utilize with SVC. This worked well almost instantly. Over time, we started to notice that through the Windows operating system, the microphone would turn off automatically for unknown reasons. We recommend turning off the audio enhancement setting under the voice properties as this inexplicably conflicted with the SVC application. After this setting was toggled off, no errors related to microphones were reported to IT. One thing to mention is that less technical MRI technologists will mute via the auxiliary microphone/audio device and will frequently call IT complaining that their microphone is not working correctly. Explaining to the technologists the process of how the external microphone and audio device works was the easiest way to remedy this minor problem.
After IT procured the correct workstations, monitors as well as external audio devices, technical trouble tickets between MRI technologists and the IT staff became a rare occurrence. Most technical issues from this point forward were strictly related to topics such as performance, technologist’s SVC credentials, and standard KVM related issues. All the issues identified above are issues your IT team needs to be comfortable managing and handling internally if SVC is to be used.
Technologist/Tech assistant approach and training
We chose a technically savvy, experienced MRI technologist as the leader of this project. It is imperative that the individual you choose to serve as the lead have the confidence and right temperament to train other staff across the organization, including all MRI technologists and MRI technologist assistants. Our technologist not only fit this bill, but he also spent extensive time testing each step of the IT setup described above.
The initial training with SVC was not difficult. Once a technologist learned how to log on and navigate the SVC interface, he had little to no difficulties because SVC is designed to mimic a technologist being at the scanner. Therefore, the key to success is that the technologist must be familiar with the magnet’s operating console. Our lead technologist spent a week at each of our centers and trained all MRI technologists and technologist assistants on how to utilize SVC.

During the deployment process, all technologists were trained on-site at their current location and virtually scanned using “their” on-site magnet. Using this training procedure, the technologists quickly became comfortable with SVC as they were merely scanning on the equipment they normally utilize. They then graduated to scanning on one magnet located at another site during their downtime. Finally, they learned to scan on their scanner and one remote MRI while that off-site MRI technologist was present at the remote location to provide feedback. After training was completed, each technologist was required to continue to utilize SVC at other deployed sites for a few cases each day, and this activity was logged and reported daily for monitoring purposes. This process not only kept the technologists in touch with the product and continued their training, so they remained comfortable with the platform, but it also assisted the IT department in testing all connections for reliability. Once the platform was deployed across the entire system, we continued utilizing SVC daily, even though there was a technologist present at that site, in order to increase our staff’s experience and comfort level with the product.
In addition to training current staff, we hired and trained additional technologist assistants on MRI safety and positioning. Technologist assistants are integral members of this team, working closely with MRI technologists to enhance patient care and imaging efficiency. Their role is vital in delivering high-quality MRI services with SVC while maintaining patient safety and ensuring seamless workflow. Technologist aides work collaboratively with MRI technologists, radiologists, and other members of the healthcare team. Effective communication and teamwork are essential for providing seamless patient care and achieving successful imaging outcomes. Protocols requiring open lines of communication were written and implemented. The intercom communication device is a critical part of the SVC system to maintain a collaborative environment. Technologist aides assist in preparing and positioning patients for MRI procedures, ensuring their comfort, monitoring patients for any signs of discomfort or anxiety, and providing reassurance and support to patients as needed. Additionally, they assist in selecting and positioning in MRI RF (Radiofrequency) coils, follow strict safety protocols, maintain accurate records of patient information, imaging procedures, and any adverse events that may occur during the MRI scan. All technologist assistants require extensive training in MRI patient positioning and safety protocols. Technologist assistants are held to a standard of knowledge that is within their scope of practice and this allows them to function as assets of patient care and preparation for the remote technologist.
We placed these new tech assistants at our busiest locations to help with patient workflow when the technologist was present, but if we experienced a technologist shortage, they would handle MRI positioning and assist with safety with the virtual technologist providing coverage. We chose to hire medical assistants or individuals with some medical experience so they could get up to speed more rapidly. Radiology assistants would be a consideration, but they are not readily available in our market. Technologists in this model are able to focus mainly on scanning while the technologist assistants handle the patients, which expedites and improves the workflow.
Once we deployed SVC at multiple sites, we used the staffing process described above to cover callouts for sickness or for vacation coverage. During this initial trial period, we asked for volunteers to cover these shifts, and no additional compensation was offered; however, once we were fully live across the system, we created a bonus structure to incentivize staff who covered two or three units.
As a matter of corporate policy, we decided that training on SVC was not optional for our MRI technologists, and it was deemed a required part of their job duties. It is important to present SVC to the technologists in a non-confrontational manner, explain that this tool is not going to replace them, and assure them that their fear that they are replacing themselves by being required to cover multiple units is unfounded. After training was completed, we began requiring “shared coverage” during the day across two sites, meaning one technologist at a given location would cover their magnet and a second magnet for half their shift, and then the second magnet’s technologist would cover both locations for the remaining half shift. This “shared coverage” model has improved morale amongst technologists as they are now only working for half the day scanning and have the remaining half day to complete other professional duties.
We experienced more skepticism than resistance from techs when it came to implementing SVC. Naturally, because technologists were unfamiliar with this new technology, it was hard for them to conceptualize how this would work in practice prior to undergoing training. The week of training was beneficial to mitigating this skepticism. Once a technologist saw SVC in use, they became more open to the idea of using SVC, especially after it was made clear that SVC would not replace them but was a tool easing their job duties. Most technologists viewed SVC as the future of MRI and wanted to be part of this leading edge experience.
Concerns about equitable compensation were also on the minds of MRI technologists. While the prospect of this technological advancement is exciting, it raises legitimate questions about compensation for MRI technologists, whose skills and expertise play a pivotal role in the success of this new approach. In recognizing the importance of addressing these concerns, MRI technologists should engage in constructive dialogues with those who oversee the organization’s compensation structure. The agreed upon solution was to provide a $20 per hour bonus to technologists scanning multiple units at one time. This acknowledged the unique demands and added responsibilities associated with multi-unit remote scanning. This compensation initiative underscored the organization’s commitment to recognizing and valuing the contributions of MRI technologists who operated multiple units. Beyond the financial incentive, it signifies an understanding of the additional complexities and challenges involved in managing multiple scans concurrently.
The above-referenced bonus structure, which comes into play when a technologist covers more than one MRI, was received very positively. Technologists were receptive to this idea, and it has been fruitful in securing successful implementation. The bonus was interpreted as fair compensation with staff understanding that they were benefiting from the services of a technologist assistant daily and that the company invested significant resources in infrastructure and their training. They, therefore, did not expect to double their salary when covering multiple magnets, but the bonus did help increase their enthusiasm and job satisfaction during implementation.
If there is a callout or vacation coverage is required, our practice managers use SVC to cover the gap. During a callout, the technologist assistant positions the patient in any coils/magnet and assists in performing the screening process. If there are any questions which arise during the positioning, the virtual tech is always available to answer them. IV placement and contrast coordination are provided by the covering radiologist, nurse practitioner, or on-site physician assistant. With SVC, we manage callouts more efficiently without interrupting the scheduled hours of operation or inconveniencing the patients.
One final function of SVC is the provision of advanced imaging, training, and technologist support. Our veteran MRI technologists easily assist with more difficult exams and provide virtual support through SVC. We utilize SVC routinely for cardiac MRIs across the system as we have a limited number of technologists comfortable with this type of imaging. In addition, this assists us when recruiting new technologists who lack experience on different types of scans because they quickly realize they have backup within our network when issues arise. This can be particularly helpful when learning a new machine.
Policies and procedures
The implementation of remote MRI scanning introduces a new dimension to patient care, enabling diagnostic procedures to be conducted with the patient at a remote site while the MRI technologist oversees the process from a central location. While this approach offers the potential for increased efficiency and broader access to MRI services, it raises legitimate questions about responsibility, accountability, and patient safety. Recognizing the gravity of these concerns, MRI technologists play a vital role in ensuring that the transition to remote scanning is seamless and safe. We engaged the MRI technologists in open dialogues with policy administrators who oversee the organization’s strategies. We also highlighted the organization’s commitment and approach to implementation which would benefit the technologists in the manner described above. This proactive approach fostered a clear understanding of how SVC would be implemented. The policies we’ve implemented since integrating SVC highlighted the organization’s commitment to providing excellent patient safety. These policies underscored the necessity of MRI technologists gaining a comprehensive understanding of the specifics regarding remote coverage, which includes scenarios such as technical malfunctions during remote scans or potential complications arising with remote patient interactions.
Additionally, MRI technologists must also grasp the nuances of remote scanning procedures, particularly in terms of adhering to established protocols and safety measures. The seamless coordination between the remotely located technologist and the on-site personnel is pivotal to ensuring that patient welfare is not compromised during the procedure. The MRI technologists and the entire team are not merely safeguarding their professional interests, but they are also upholding their ethical responsibility towards patient well-being. This approach is characterized by a commitment to the highest standards of care, regardless of whether procedures are conducted in-person or remotely. A well-informed technologist is better equipped to make informed decisions that prioritize patient safety and contribute to the organization’s overall risk management strategy.
Existing policies were edited to include SVC and additional policies were developed and implemented to address concerns arising from the use of SVC. Practices interested in using SVC should consider revising or developing new policies to address the following topics: MR Safety, MR Coils and Handling, Patient Screening, Patient Preparation and Positioning, Emergency Protocol and Action, MR Emergency Stop Procedures at the Console, Virtual Cockpit Access Procedures, Patient Privacy and HIPAA.
Communicating the changes to existing policies and notifying staff about new policies is a crucial part of deployment. Step by step screen shot images of the process were included when appropriate in the policies. Examples of policies which should be considered in such are deployment are the following:
1. SVC Requirements and Guidelines;
2. SVC Safety Considerations and System Failure Protocol;
3. SVC Enabling Connection;
4. SVC Steering Workstation Workflow and Utilization;
5. SVC Case Logs;
6. MRI Technologist Training Checklist and Sign Off;
7. Technologist Assistant Training Checklist and Sign Off; and
8. SVC Compensation Form.
We-Scan implementation
We also deployed We-Scan, which leverages the traditional Siemens Remote Service (SRS) infrastructure to get connected into our environment. Once SRS is successfully authenticated and connected, remote Siemens-provided technologists will be placed onto a secure virtual SVC terminal at a designated location from which they will perform their MRI scan duties. From the tech’s perspective, it feels as if he/she is sitting on a terminal at our physical locations. The Siemens-provided technologist will work with a technologist assistant who is on-site to handle patient positioning and MRI screening/safety. The WeScan technologists can scan on three MRI units simultaneously, and this complements our existing infrastructure and leverages previously explained design considerations.
In our tight job market, we had trouble staffing technologist coverage after normal business hours and on the weekend; therefore, we chose We-Scan to provide coverage during the hours of 7 am to 9 pm Monday through Friday, and from 8 am to 5 pm on Saturday. This additional solution was viewed as a method of optimizing the available technologists and maximizing hours of operation.
In our organization, most scanners in use are manufactured by Siemens, of which there were at least seven different platforms/models. In addition to Siemens, we also use Hitachi, Fonar, and GE scanners. When interviewing a We-Scan technologist candidate offered by Siemens, our primary concern was ensuring that the individual had significant Siemens experience and a willingness to learn the Hitachi and GE systems.
During the hiring process, Siemens provided the organization with several We-Scan technologist candidates to interview and review. Resumes were initially provided and reviewed, and Siemens arranged the virtual interviews, which were conducted by two of our senior managers. In total, we conducted six interviews, several of which declined our offer due to taking other assignments. The candidates were interviewed utilizing standardized questions about experience, knowledge, and exam protocols, as well as some behavioral questions. All interviewed candidates had significant Siemens experience and either had experience with other manufacturers or were willing to learn.
Siemens ensured that the candidate who was selected would be able to scan on all Siemens units regardless of the platform. Once we identified a candidate, that individual attended the Siemens “bootcamp” program which typically requires six weeks to complete. Another consideration which was critical to ensure We-Scan’s success is the IT department’s involvement and testing of these candidates prior to hiring.
Management would strategically utilize We-Scan technologists to expand hours at facilities and assist in coverage of open shifts throughout the system. The goal was to provide additional night and weekend coverage at locations that were previously not open during those hours. The schedule for We-Scan was set up as a separate schedule from our regular MRI technologist schedule. We also created a policy to be distributed to imaging center staff on the We-Scan process.
Patient satisfaction
Patient reaction and reception to the presence of a remote operator has been overwhelmingly positive. Utilizing a virtual technologist assistant allows on-site staff more face time with the patient as they have no scanning responsibility. Most patients are focused on getting in and get out as quickly as possible when it comes to getting their MRI and efficiency and competency is of the upmost importance.
Discussion
The landscape of healthcare is marked by a constant quest for innovation and efficiency, and the realm of medical imaging is no exception. However, as this paradigm shift unfolds, virtual medicine has come to the forefront of accepted patient care. SVC allows an MRI technologist to operate multiple MRI units from a single location. As a result, we have enhanced operational efficiency, improved patient care, optimized resource allocation, and solved challenges related to staffing including covering planned personal and unplanned sick time. By leveraging these advanced technologies and streamlined workflows, healthcare facilities can benefit from increased productivity and reduced downtime, ultimately leading to a more effective and resilient medical imaging department. These crucial components and the program’s ability to expand the knowledge of MRI technologists contribute to SVC’s overall success.
The process of implementation required us to ensure that network traffic would not be adversely affected and there would be no lag in video and response time while scanning remotely. Also, we ensured that we had reliable network connections so that the possibility of network or hardware/software failure is minimized. Although the technical considerations and needs during implementation were significant, with an experienced IT team, implementation can be easily achieved. In retrospect, a KVM deployment across all vendors, including Siemens units running Expert-I, would be the most seamless approach. The latencies achieved with this method were more favorable than using Expert-I. An in-depth assessment of your existing MRI systems is require as typical KVM outputs are being phased out and being replaced by fiber optics. Alternative “modern” KVM switches would need to be utilized in such scenarios, although a simple work around option would be to use Expert-I on those machines.
We experienced such a scenario on the next step of our SVC deployment, which involved our CT fleet. Since our most recently deployed units have only fiber inputs/outputs, KVM deployment was not an option. This is only one of many additional hurdles of SVC deployment on this modality. Other considerations to keep in mind are licensure, machine triggering, and contrast, all of which, once addressed, will benefit our delivery and coverage across our CT units.
Technologist and technologist assistant training and coverage was critical to the successful implementation of SVC. Our multi-step approach to training and rollout ensured patient safety and maximized technologist satisfaction with the product. The compensation bonus structure served as an incentive and tangible acknowledgment of their skills in adapting to the new system and maintaining the highest standard of patient care. This reflects a strategic alignment between technological advancement and recognizing the human component of healthcare delivery. We found these motivated technologists to embrace change and contribute to continuous improvement.
The challenges to implementation of SVC are costs, IT support, and technologist acceptance. Costs of implementation consist of additional salaries of technologist assistants, the investment in IT infrastructure, the bonus structure for technologists, and the cost of SVC software. The IT support needed is considerable but most experienced network engineers can implement the product with the support of the vendor.
Technologist acceptance is important to address early in the process so that resistance is limited. In our experience, technologists embraced the new technology when it was implemented properly.
Declarations
Data statement: The author declare that they had full access to all of the data in this study and the author take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding: None.
Ethical statement: The author reports this is my original research and presents an accurate account of the work performed as well as an objective discussion of its significance. All data is represented accurately in the paper.
The author has written entirely this original work.
Authorship is limited to those who have made a significant contribution to the conception, design, execution, or interpretation of the reported study. All those who have made substantial contributions are listed as the author.
No generative AI and AI-assisted technologies in scientific writing was utilized for this article.
Summary sentence
SVC can be implemented successfully across a wide geography to provide redundancy in a health system to improve patient care.
References
- Bureau of Labor Statistics, U.S. Department of Labor, Occupational Outlook Handbook, Radiologic and MRI Technologists, at https://www.bls.gov/ooh/healthcare/radiologic-technologists.htm
- Radiol Manage. 1990; 12(1): 20-6.
- Becker’s Hospital Review Staffing shortages by state. 2022. Staffing shortages by state (beckershospitalreview.com)
- Siemens Healthineers. syngo Virtual Cockpit - Siemens Healthineers (siemenshealthineers.com)
- Siemens Healthineers. We-Scan - Remote Scanning for MR Imaging - Siemens Healthineers (siemens-healthineers.com).