
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
A unique case of unresectable metastatic gastric squamous cell carcinoma treated with combined nivolumab and capecitabine/oxaliplatin complicated by immunotherapy induced pure red cell aplasia
Amith Rao1*; Umbreen Rozell2; Junaid Arshad2
1Department of Internal Medicine, Banner University Medical Center, Tucson, AZ 85719, USA.
2Department of GI Oncology, University of Arizona Cancer Center, Tucson, AZ 85719, USA.
*Corresponding Author: Amith Rao
Department of Internal Medicine, Banner University
Medical Center, Tucson, AZ 85719, USA.
Email: raoa@arizona.edu
Received : Apr 11, 2024
Accepted : May 01, 2024
Published : May 08, 2024
Archived : www.jclinmedimages.org
Copyright : © Rao A (2024).
Abstract
Gastric Squamous Cell Carcinoma is an extremely rare type of gastric cancer, with an incidence of 0.04-0.07% among all gastric cancers [1]. The treatment for this malignancy has focused on surgical resection with adjuvant chemotherapy. Treatment for unresectable metastatic disease has varied, with most regimens taken from management of traditional gastric adenocarcinoma and other GI malignancies with varied success. Here, we will explore a case of a patient diagnosed with metastatic gastric squamous cell carcinoma treated with combination nivolumab and capecitabine with oxaliplatin regimen having a complicated course involving medication induced pure red cell aplasia.
Keywords: Gastric squamous cell carcinoma; Pure red cell aplasia; Oxaliplatin; Nivolumab.
Citation: Rao A, Rozell U, Arshad J. A unique case of unresectable metastatic gastric squamous cell carcinoma treated with combined nivolumab and capecitabine/oxaliplatin complicated by immunotherapy induced pure red cell aplasia. Open J Clin Med Images. 2024; 4(1): 1182.
Introduction
Gastric cancer is the third leading cause of cancer-related death globally, with 95% of gastric cancers classified as adenocarcinoma, followed by primary gastric lymphoma [2]. Risk factors for cardia-related (opening of GE junction) gastric cancers are primarily obesity and GERD, however, non-cardia related gastric cancers are more prevalent in patients with H.pylori infection, poor socioeconomic factors, and diet (smoking/alcohol use) causing chronic gastritis [2]. Primary gastric squamous cell carcinoma accounts for <1% of all cases worldwide with fewer than 100 cases reported across the globe [3]. The incidence has been documented more in Japan, notable for high rates of gastric cancer due to increased H-pylori infection rates associated with frequent consumption of salty and smoked foods. A case series review of 56 patients in Japan has shown Primary Gastric Squamous Cell Carcinoma (PGSCC) to be more common in men than women (5:1 ratio) [4]. The location of this malignancy has been variable, with the highest incidence being centered on the upper one third of the stomach (50%) [4]. The average depth of invasion on diagnosis has been T4a or T4b in over 50% of cases, making surgical resection a poor option even in cases of relatively localized disease. No consensus has been reached on how to treat metastatic unresectable gastric squamous cell carcinoma, as previous regimens utilizing more conventional gastric adenocarcinoma and squamous cell carcinoma regimens have met with limited success [4]. This case will explore a potentially successful management of metastatic gastric squamous cell carcinoma utilizing immunotherapy and will illustrate a rare but significant side effect of immunotherapy.
Case presentation
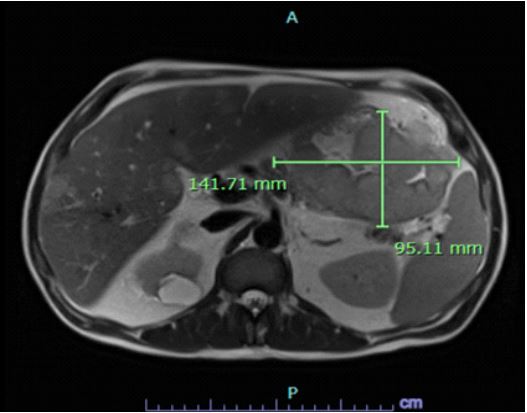
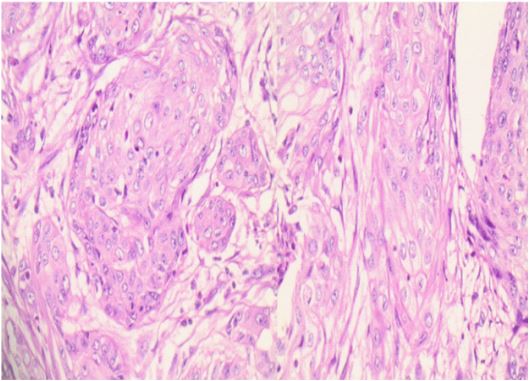
We present the case of a 53-year-old male with past medical history of hypertension, alcohol abuse, left forearm/hand cellulitis who initially presented to the emergency department with generalized abdominal pain, nausea, vomiting for 3 weeks prior to presentation. The patient also reported bloating sensation and a pulling sensation in his abdomen. The patient denied any history of smoking, or alcohol use, or any family history of malignancy. Laboratory results were significant for white Blood Cell Count (WBC) of 36.5 with left shift (neutrophils 32.61 k/ uL), hemoglobin of 6.8 g/dL, hematocrit of 23.8%L, platelets of 499 k/uL, and elevated alkaline phosphatase of 245 IU/L. MR abdomen and pelvis showed a 9.5 cm x 14.1 cm mass arising from the greater curvature of the gastric body. The patient underwent endoscopic ultrasound with biopsy; pathology showed squamous cell carcinoma of gastric origin (Figure 2). MRI abdomen and pelvis also showed hepatic and bone metastases. The patient was evaluated by surgical oncology team and was deemed not a surgical candidate in setting of metastatic disease. The patient underwent Next Generation Sequencing (NGS) on the tumor sample which showed the tumor cells to be positive for Program Death Ligand (PD-L1) with a Combined Proportion Score (CPS) of 95, CK5+, P40+, and CDX2+. Staining was negative for CK7 and IS EBER (immunostaining of Epstein Bar encoding region).
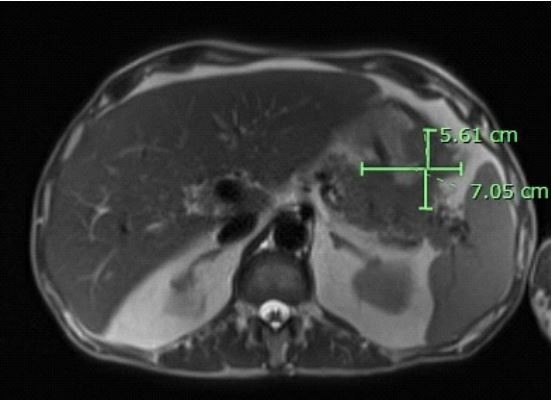
The patient was started on combined Capecitabine and Oxaliplatin (CapeOX) chemotherapy along with nivolumab (anti PD-1 inhibitor) for management of unresectable metastatic gastric squamous cell carcinoma. The patient finished 7 cycles of treatment with repeat MR abdomen and pelvis showing decrease in size of gastric mass to 5.6cm x 7.1 cm (Figure 2). The patient had no severe side effects to this point with only asymptomatic stable anemia (Hb 7-8).
The patient was hospitalized after the 7th cycle of CapeOX and nivolumab for concerns of symptomatic anemia (referred from cancer center due to hemoglobin of 6). EGD and CT abdomen pelvis were both negative for acute bleed. The patient had hemolysis workup (LDH, haptoglobin, Direct Antiglobulin Test (DAT), peripheral blood smear) and infectious workup (parvovirus, HIV, EBV, Hep B/C) which revealed no obvious cause. The patient also had bone marrow biopsy performed inpatient which showed reduced red cell precursors with some inclusion bodies and increased myeloid: nucleated erythroid ratio (6:1). The patient was discharged home after 72 hours of stable hemoglobin prior to bone marrow biopsy results, returned to ED 2 weeks later for symptoms of lightheadedness/dizziness with hemoglobin of 4.5. The patient continued to require frequent blood transfusions during hospitalization, with the concern for possible Pure Red Cell Aplasia (PRCA). The patient’s hemolysis workup and infectious workup as above was repeated which revealed no obvious cause. After review of the medication list and in the setting of no other clear etiology, nivolumab was implicated as cause of PRCA and was held. The patient was started on 1 mg/kg prednisone inpatient for treatment of PRCA and showed improvement in hemoglobin levels to above 7 with slow taper of prednisone regimen over 6-8 weeks. Repeat bone marrow biopsy done 1 month after hospitalization showed resolution of PRCA on prednisone regimen; this supported diagnosis of nivolumab induced PRCA.
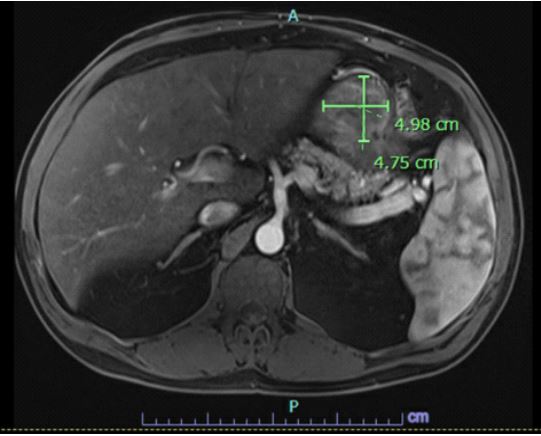
The patient was restarted on CapeOX therapy, completed 9 additional cycles without nivolumab with no progression of disease, however repeat MR abdomen pelvis prior to 10th cycle showed progression in size of mass 4.98 x 4.75 cm compared to 3.6 x 3.5 cm by the prior CT (Figure 4).
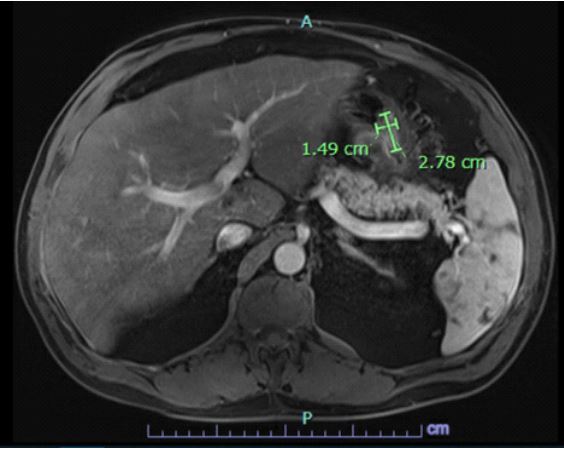
Based on degree of progression, the decision was made to switch the patient to carboplatin and paclitaxel (standard of care for typical squamous cell carcinomas). Hepatobilliary and radiation oncology were consulted regarding further surgical/ radiation treatment, stated will re-evaluate based on efficacy of new regimen in reducing the size of the tumor. Repeat MR abdomen and pelvis after 3 cycles showed improvement in mass to 2.78 x 1.49 cm when compared to previous MR abdomen with mild interval improvement in size of hepatic metastatic lesions (Figure 5).
The plan is to continue carboplatin plus paclitaxel until disease progression or unacceptable toxicity with serial scans and monitoring and follow-up with radiation oncology and surgery regarding possible surgical resection of mass given interval improvement. Immunotherapy will continue to be held.
Discussion
This case illustrates a presentation of a rare malignancy and the challenges associated with management with initial success with a combined capecitabine-oxaliplatin regimen with nivolumab. This patient presented with a mass extending from the greater curvature of the stomach with no classic presenting risk factors (no history of H. pylori, no history of smoking or drinking), and symptoms were present only with in the 3 weeks prior to presentation. It has been theorized that primary gastric SCC often appears to have a poorer prognosis due to a higher rate of lymphovascular invasion and metastasis on diagnosis than traditional gastric adenocarcinoma, however, this claim remains unproven considering a very limited sample size of available cases [5].
There is a lack of studies specifically into Primary Gastric Squamous Cell Carcinoma (PGSCC) regarding the efficacy of immunotherapy, however studies have shown significant response with nivolumab in metastatic gastric adenocarcinoma [6]. The patient’s PD1-recepter expression (CPS score) was elevated, allowing for the use of nivolumab as therapy. Prior tried regimens for metastatic PGSCC have centered around combination chemotherapy with capecitabine and FOLFOX or mFOLFIRI with poor outcomes and a limited sample size [7]. The patient showed marked response to the combined chemotherapy and immunotherapy regimen initially with limited side effects, as the size of the primary tumor shrunk to over 50% of its original size with improvement in clinical symptoms. The success of this regimen supports using next generation sequencing in all cases of PGSCC for potential PD-1 inhibitor use as a combination with chemotherapy.
The overall efficacy of this regimen however is complicated by the adverse event of pure red cell aplasia, as the nivolumab needed to be stopped after 7 cycles. The safety profile of this combined regimen was explored in a separate trial analyzing efficacy of capecitabine + oxaliplatin and nivolumab in advanced gastroesophageal, esophageal, and gastric adenocarcinoma [6]. The most common side effects associated with this combined regimen were nausea, diarrhea, and peripheral neuropathy (occurred roughly 25% of the time) [6]. Grade 3 anemia (defined as Hb 6.5-8) occurred in 6% of patients on the combination therapy, and Grade 4 anemia (defined as Hb <6.5) occurred in less than 1% of patients [6]. The trial did not directly define patients who developed PRCA from the combination therapy. The patient in this case did have Hb between 7-8 (Grade 3) for most of the treatment course, and only progressed to Grade 4 after 7 cycles of combined nivolumab and CapeOX therapy. Single agent nivolumab has been shown in package inserts to cause Grade 3/4 anemia 2.8% of the time in prior studies [6].
The mechanism of PRCA secondary to immunotherapy is not currently well understood. PRCA has been shown in laboratory studies to have mechanisms that are both antibody related, and T-cell mediated. Autoimmune disease processes (lupus, rheumatoid arthritis, autoimmune hemolytic anemia) have been shown to have a primarily antibody mediated mechanism, with immunoglobulins inhibiting production of red cell precursors resulting in acquired PRCA [8]. However, PRCA secondary to more lymphoproliferative causes (chronic lymphocytic leukemia, diffuse large B cell lymphoma, Human T-cell lymphotropic virus type 1) appears to be more T-cell mediated, with activation of CD4/CD8+ T-cells and Natural Killer (NK) cells that limit erythropoiesis by killing erythroid colony units and burst colony forming units, both of which are integral to production of mature erythroblasts in the marrow [8]. Nivolumab’s mechanism of action is T-cell mediated, as it acts as a synthetic PD-1 monoclonal antibody that binds to PD-1 receptors on T-cells and prevents binding of the PD-L1 and PD-L2 molecules produced by tumor cells which typically suppresses further T-cell activation [9]. This consequently results in an increased T cell response, which theoretically works in a similar manner to lymphoproliferative processes to destroy progenitor units in the marrow.
It is still unclear as to why this effect happened in this patient who was on a combined regimen of capecitabine +oxaliplatin with nivolumab. One logical explanation is connected to oxaliplatin, which has been shown in literature to increase production of cytotoxic CD8+ T-cells [10]. Studies have also shown that STAT3 mutated CD8+ T cells influence selective inhibition of erythroid progenitors in PRCA patients [11]. Based on this, it is possible that increase in proportion of CD8+ T cells due to combined oxaliplatin and nivolumab therapy may have resulted in excess inhibition of marrow erythropoiesis leading to PRCA. This is only a theory, however, as mutation receptor analysis was not done in this patient, and more thorough analysis needs to be done to elucidate the mechanism behind immunotherapy-induced pure red cell aplasia as the answer is likely multifactorial.
Regarding treatment of PRCA, the first line treatment is centered on addressing the underlying cause of the disease process. In this case, the cause was likely secondary to immunotherapy, and the drug was discontinued. The patient continued to require refractory transfusions inpatient for the next 2 weeks, and the decision was made to pursue immunosuppression. The first line therapy for PRCA in non-immune related PRCA with greatest efficacy is cyclosporine A , which has shown a response rate of 75-80% in patients in 4-8 weeks [12]. However, in immunotherapy related PRCA, prednisone has been considered first line, and this regimen was used in this patient with resolution of symptoms upon repeat bone marrow biopsy in 4 weeks. When considering the mechanism of action of the two immunosuppressive regimens, however, it is interesting to note that cyclosporine has more of a direct effect on inhibition of T-cell production, which may be beneficial in this context if operating under the assumption of nivolumab related PRCA being a T-cell mediated process.
Conclusion
This case illustrates a rare presentation of unresectable metastatic gastric squamous cell carcinoma treated with combined capecitabine + oxaliplatin and nivolumab regimen with significant initial success on the combined regimen. The patient also demonstrated stability for a period on CapeOX without nivolumab, however eventually had disease progression requiring a switch to carboplatin/paclitaxel. This case provides more insight into how to manage this rare malignancy and invites more research to corroborate the efficacy of this regimen. This case also outlines a rare but a challenging side effect of nivolumab and reinforces the need for close monitoring, cessation of immunotherapy, and prompt treatment if high clinical suspicion for pure red cell aplasia. Further studies need to be done to analyze the efficacy of a combined chemotherapy/immunotherapy regimen vs established chemotherapy regimens in unresectable metastatic gastric squamous cell carcinoma and to elucidate the mechanism behind immune checkpoint inhibitor related pure red cell aplasia.
References
- Gonzalez-Sanchez JA, Viton R, Collantes E, Rodriguez-Montes JA. Primary Squamous Cell Carcinoma of the Stomach. Clin Med Insights Oncol. 2017; 11: 1179554916686076. doi:10.1177/1179554916686076.
- Rawla, P, Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz Gastroenterol. 2019; 14: 26-38, doi:10.5114/pg.2018.80001.
- Vailas MG, Syllaios A, Hasemaki N, Sotiropoulou M, Mpaili E, et al. A type of neoplasia deadlier than gastric adenocarcinoma? Report of a case of primary gastric squamous cell carcinoma. World J Surg Oncol. 2019; 17: 113. doi:10.1186/s12957-019-1657-x.
- Wakabayashi H, Matsutani T, Fujita I, Kanazawa Y, Nomura T, et al. A rare case of primary squamous cell carcinoma of the stomach and a review of the 56 cases reported in Japan. J Gastric Cancer. 2014; 14: 58-62. doi:10.5230/jgc.2014.14.1.58.
- Volpe CM, Hameer HR, Masetti P, Pell M, Shaposhnikov YD, et al. Squamous cell carcinoma of the stomach. Am Surg. 1995; 61: 1076-1078.
- Janjigian YY, Shitara K, Moehler M, Garrido M, Salman P, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet. 2021; 398: 27-40. doi:10.1016/S0140-6736(21)00797-2.
- Guzman Rojas P, Parikh J, Vishnubhotla P, Oharriz JJ. Primary Gastric Squamous Cell Carcinoma. Cureus. 2018; 10: e2389. doi:10.7759/cureus.2389.
- Balasubramanian SK, Sadaps M, Thota S, Aly M, Przychodzen BP, et al. Rational management approach to pure red cell aplasia. Haematologica. 2018; 103: 221-230. doi:10.3324/haematol.2017.175810.
- Rendon A, Rayi A. Nivolumab. In StatPearls; Treasure Island (FL). 2024.
- Stojanovska V, Prakash M, McQuade R, Fraser S, Apostolopoulos V, et al. Oxaliplatin Treatment Alters Systemic Immune Responses. Biomed Res Int. 2019; 2019: 4650695. doi:10.1155/2019/4650695.
- Kawakami T, Sekiguchi N, Kobayashi J, Imi T, Matsuda K, et al. Frequent STAT3 mutations in CD8(+) T cells from patients with pure red cell aplasia. Blood Adv. 2018; 2: 2704-2712. doi:10.1182/bloodadvances.2018022723.
- Gurnari C, Maciejewski JP. How I manage acquired pure red cell aplasia in adults. Blood. 2021; 137: 2001-2009. doi:10.1182/blood.2021010898.