
Open Journal of
Clinical and Medical Images
Research Article - Open Access, Volume 4
Immunoglobulin G4-related sclerosing cholangitis
Yu-Bao Xue1†; Rong-Xin Xie1†; Xin-Yu CI2; Mei-Juan Zhang3*
1Department of Gastroenterology, Shandong Provincial Qianfoshan Hospital, Shandong First Medical University, No. 16766 Jingshi Road, Jinan, Shandong, 250014, China.
2Department of Gastroenterology, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, No.16766 Jingshi Road, Jinan, Shandong, 250014, China.
3Department of Health Management, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Engineering Laboratory for Health Management, No. 16766 Jingshi Road, Jinan, Shandong, 250014, China.
†Yu-bao Xue and Rong-Xin Xie Contributed Equally to this Manuscript.
*Corresponding Author: Mei-Juan Zhang
Department of Health Management, The First Affiliated
Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Engineering Laboratory for Health Management, No.16766
Jingshi Road, Jinan, Shandong, 250014, China.
Email: meijuanzhang@126.com
Received : Apr 11, 2024
Accepted : May 06, 2024
Published : May 13, 2024
Archived : www.jclinmedimages.org
Copyright : © Mei-Juan Z (2024).
Abstract
Aims: The purpose of the review is to summarize the clinical features of Immunoglobulin G4-related sclerosing cholangitis.
Methods: PubMed was searched with the following search terms: “Immunoglobulin G4-related sclerosing cholangitis” “IgG4- SC”. Analyze its possible etiology, summarize its clinical features and treatment.
Results and conclusion: A total of 118 cases of sclerosing cholangitis associated with IgG4 were reported. More than half of the patients were from Asia, with a male to female ratio of about 4.6:1. Jaundice and abdominal pain are the most common clinical manifestations, and some patients may have yellow skin scleral staining. Elevated IgG4 occurred in 70 patients, and abnormal liver function was the most common occurrence on hematological tests. Most patients will have different degrees of bile duct stenosis, bile duct dilatation, biliary wall thickening and other manifestations in the imaging examination. Most patients received corticosteroid therapy, a small number of patients received surgical treatment, some patients also used anti-tumor drugs and immunosuppressants, combined with anti-infection, gallbladder, liver protection and symptomatic supportive treatment. Most patients recover well after combined treatment, but a few eventually die from other serious complications.
Keywords: Immunoglobulin G4-related sclerosing cholangitis (IgG4-SC); Clinical features.
Citation: Yu-Bao X, Rong-Xin X, Xin-Yu CI, Mei-Juan Z. Immunoglobulin G4-related sclerosing cholangitis. Open J Clin Med Images. 2024; 4(1): 1183.
Introduction
IgG4-related diseases are a group of conditions that are identified by high levels of IgG4 in the blood, the presence of numerous IgG4-positive lymphocytes and plasma cells in affected tissues, and fibrosis. These diseases can affect various organs in the body, such as the biliary tract, liver, gastrointestinal tract, pancreas, lacrimal glands, salivary glands, central nervous system, thyroid, lung, kidney, prostate, retroperitoneal area, skin, breast, arteries, and lymph nodes. IgG4-SC is a manifestation of IgG4-RD biliary tract involvement. It tends to occur in older men, with or without autoimmune pancreatitis. Patients with IgG4-SC present with obstructive jaundice and abdominal pain, along with significantly elevated serum IgG4 levels. They also exhibit segmental or diffuse intrahepatic and/or extrahepatic bile duct stenosis, bile duct wall infiltration with a large number of IgG4-positive plasma cells and lymphocytes, and extensive fibrosis. The imaging features of IgG4-SC are similar to those of Primary Sclerosing Cholangitis (PSC), pancreatic cancer, and cholangiocarcinoma. Preoperative diagnosis is difficult, especially when proximal bile duct IgG4-SC occurs alone. This summary of IgG4-SC characteristics provides a reference for diagnosis, treatment, and subsequent management of the disease.
Methods
The data for this study were collected by searching PubMed using the following keywords: ‘IgG4-related sclerosing cholangitis’, ‘IgG4-SC’, ‘IgG4’, and ‘cholangitis’. The study’s inclusion criteria were as follows: full-text case reports or series of patients with a possible diagnosis of IgG4-related cholangitis based on the four diagnostic criteria developed by the 2012 Japan Research Committee on IgG4-Related Diseases and the Hepatobiliary Refractory Diseases Research Committee, or with a possible diagnosis of IgG4-related cholangitis that is available online without any restrictions on the date of publication. The exclusion criteria for this study include duplicate publications, lack of access to full text, lack of permission to download, and review articles. There is no time limit for data collection. A search of the specified databases yielded a total of 137 articles. Ninetyfive eligible literature (case reports/series) were reviewed, and the following data were extracted: (1) sex, (2) age, (3) country, (4) clinical manifestations, (5) past history, (6) family history, (7) signs, (8) ancillary test results, (9) treatment, and (10) prognosis. A total of 118 cases were reported in the 95 relevant literature as of the date of preparation (30 May 2023).
Result
Clinical characteristics
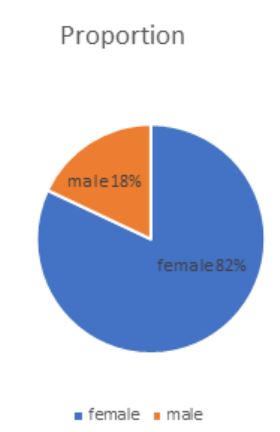
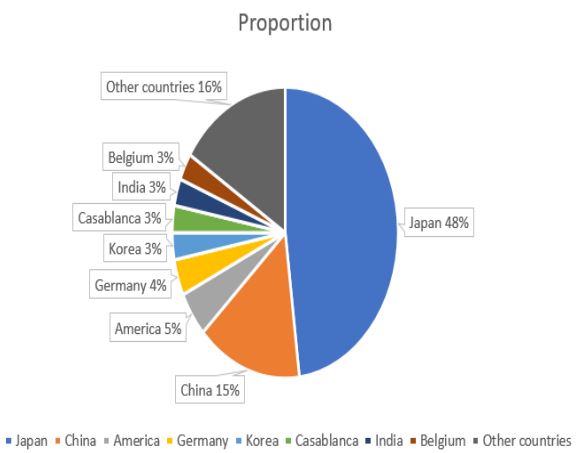
Out of the 118 patients (Figure 1), 21 were female (18%) and 97 were male (82%), resulting in a male-to-female ratio of approximately 4.6:1. The age range of the patients was between 13 and 87 years, with two patients not disclosing their age. The patients were from the following countries (as shown in Figure 2): Japan (n=56), China(n=18), USA (n=6), Germany (n=4), South Korea (n=4), Casablanca (n=4), India (n=4), Belgium (n=3), and other countries [including Spain (n=2), Australia (n=2), France (n=2), Netherlands(n=2), Vietnam (n=1), Israel (n=1), Denmark (n=1), Thailand (n=1), Nepal (n=1), UK (n=1), Turkey (n=1), Italy(n=1), Argentina (n=1), Poland (n=1), Norway (n=1)].
Clinical symptoms
Out of the 118 patients, 11 did not mention any clinical manifestations. The remaining 107 patients were asymptomatic, which was determined through physical examination of cholestasis, bile duct dilation, liver biochemical abnormalities, or biliary strictures. Asymptomatic patients accounted for 14% (15/107) of the total. More than half of the patients had abnormal bilirubin metabolism, which accounted for 60.75% (65/107). Jaundice was the most common symptom among patients (58.88%, 63/107), followed by itchy skin (14.95%, 16/107), dark urine or black urine (9.35%, 10/107), and lighter stool (4.67%, 5/107). Abdominal symptoms were present in 33 patients, accounting for 30.84% (33/107); the majority of patients experienced abdominal pain (20.56%, 22/107), while others had diarrhea (4.67%, 5/107), abdominal distension (2.80%, 3/107), or abdominal discomfort (2.80%, 3/107). Twenty-three patients developed systemic symptoms, including weight loss (22.43%, 24/107), fever (8.41%, 9/107), and fatigue (14.02%, 15/107). Additionally, other symptoms were reported, such as loss of appetite or anorexia (6.54%, 7/107), rash (0.93%, 1/107), loss of smell and dry eyes (0.93%, 1/107), hearing impairment (0.93%, 1/107), dyspnea (0.93%, 1/107), and enlarged pancreatic and mandibular lymph nodes (0.93%, 1/107). One patient presented with swelling of the left upper eyelid, protrusion of the left eye, limited eye movement, visual field defects, bilateral lacrimal gland swelling, and swelling of the right salivary gland. Another patient exhibited clinical and biochemical signs and symptoms of exocrine and endocrine pancreatic dysfunction. The study found that some patients exhibited positive signs, with xanthochromia of the skin and/or sclera being the most common, accounting for 17.80% (21/118). It is worth noting that 1 patient had skin scratches and 1 patient had skin peeling. Additionally, patients presented with abdominal tenderness (8.47%, 10/118), hepatomegaly (3.39%, 4/118), fever (1.69%, 2/118), lung cracks (0.85%, 1/118), and decreased breath sounds (0.85%, 1/118). One patient also developed positive ocular signs, including visual field defect and left eye dyskinesia. The percentage of symptoms (Table 1) and signs (Table 2) are summarized as follows.
Table 1: Different symptoms and percentage summary.
| Symptoms | Number and percentage |
|---|---|
| Jaundice | 63 (58.88%) |
| Weight loss | 24 (22.43%) |
| Abdominal pain | 22 (20.56%) |
| Itchy skin | 16 (14.95%) |
| Fatigue | 15 (14.02%) |
| Dark or black urine | 10 (9.35%) |
| Light stools | 5 (4.67%) |
| Diarrhea | 5 (4.67%) |
| Bloating | 3 (2.80%) |
| Abdominal discomfort | 3 (2.80%) |
| Fever | 9 (8.41%) |
| Loss of appetite or anorexia | 7 (6.54%) |
| Rash | 1 (0.93%) |
| Dry eyes and loss of smell | 1 (0.93%) |
| Hearing impairment | 1 (0.93%) |
| Dyspnea | 1 (0.93%) |
| Pancreatic enlargement | 1 (0.93%) |
| Mandibular lymphadenopathy | 1 (0.93%) |
| Eye symptoms | 1 (0.93%) |
| Pancreatic dysfunction | 1 (0.93%) |
Table 2: Summary of positive signs and percentages.
| Signs | Number and percentage |
|---|---|
| Xanthochromia of the skin and/or sclera | 21 (17.80%) |
| Abdominal tenderness | 10 (8.47%) |
| Hepatomegaly | 4 (3.39%) |
| Fever | 2(1.69%) |
| Lung cracks | 1 (0.85%) |
| Decreased breath sounds | 1 (0.85%) |
| Ocular signs | 1 (0.85%) |
Laboratory indicators
Out of the 118 patients, 80 were monitored for IgG4 concentrations. Among them, 10 had IgG4 concentrations within the normal range, while 70 had elevated IgG4 concentrations ranging from 140-7859 mg/dL, accounting for 59.32% (70/118). Abnormal liver function was observed in 79 cases, with 65 cases showing increased aminotransferase, 66 cases showing increased alkaline phosphatase, 55 cases showing increased bilirubin, 49 cases showing increased gamma-glutamyl transpeptidase, and 2 cases showing decreased albumin. In 16 cases, the white blood cell count increased, while in 11 cases, the hemoglobin decreased. Additionally, the red blood cell count decreased in 1 case, and the platelet count decreased in 1 case. The CA19-9 increased in 28 cases, CEA increased in 7 cases, and AFP increased in 1 case. There were 14 positive antinuclear antibody, 2 positive ANA, 1 positive biliary duct antibody, and 1 positive smooth muscle antibody. Amylase increased in 6 cases, and lipase increased in 3 cases. The urine sugar was positive in 3 cases. In 9 cases, CRP levels increased, while erythrocyte sedimentation rate increased in 5 cases. Lactate dehydrogenase levels increased in 3 cases, lipid levels increased in 2 cases, and fecal elastase levels decreased in 2 cases. One case showed an increase in fasting blood glucose, rheumatoid factor, and direct Coombs test. Additionally, hepatitis B core antibody, anti-HCV antibody, thyrotropin, and hyponatremia were found in this case. Free thyroxine was decreased in this case as well.
Ancillary examination
Out of the 118 patients, 87 underwent an abdominal CT examination. Among them, 38 had biliary dilatation, 32 had biliary wall thickening, 29 had biliary stenosis (including 5 cases of biliary obstruction), 15 had pancreatic enlargement, 7 had a biliary low-density mass, 6 had a pancreatic mass (including 3 tumors), 4 had pancreatic duct dilatation, and 4 had a liver lowdensity mass. The study identified several medical conditions among the patients, including 3 cases of hilar/pancreatic lymph node enlargement, 3 cases of chronic pancreatitis, 3 cases of kidney tumor, 2 cases of hilar space occupying, and 2 cases of cholestasis. Additionally, some patients presented with autoimmune pancreatitis, uneven pancreatic density, portal vein occlusion, pelvic adenomyopathy, splenic vein stenosis, abdominal aortic wall thickening, gallstones, pancreatic calcification, and hepatomegaly.
Ultrasonography was performed on 51 patients, including abdominal, endoscopic, and parotid ultrasonography. Of these patients, 28 showed thickening of the bile duct or gallbladder wall, 17 had bile duct dilatation, 15 had abnormal echo of the bile duct wall or gallbladder wall, 8 had a pancreatic or bile duct mass, 4 had hypoechoic pancreas (indicating tumor or autoimmune pancreatitis), and 3 had pancreatic enlargement. The patient presented with multiple conditions including portal vein and mesenteric vein thrombosis with iliac fossa abscess, supravicular, neck, axillary, and groin lymph node enlargement, Glissonean sheath and umbilical portal blood flow disruption, liver uneven echo, submandibular gland enlargement, chronic cholecystitis, and gallstone.
Out of the 58 patients who underwent Endoscopic Retrograde Cholangiopancreatography (ERCP), 46 had bile duct stenosis. Among them, 14 also had varying degrees of dilation of the proximal bile duct, and 7 had pancreatic duct stenosis.
A total of 42 patients underwent MRCP examination, out of which 28 showed bile duct stenosis/obstruction, 21 had bile duct dilatation, and some patients were accompanied by pancreatic duct dilatation (3 cases) and stenosis (2 cases).
PET-CT examination was performed on 15 patients, revealing abnormal uptake of 18-fluorodeoxyglucose in several locations including the liver, spleen, pancreatic duct, pancreas, various biliary ducts, mediastinum, superior phrenic lymph nodes, subphrenic lymph nodes, submandibular lymph nodes, and related tumors.
Eleven endoscopic examinations were carried out. Of these, three showed chronic atrophic gastritis, three showed no obvious abnormalities, two showed colon polyps, two showed pathological evidence of ulcerative colitis, one showed multiple ulceration of the colon, and one showed pancreatic enlargement and edema.
Treatment and outcome
Out of the 118 patients, 9 did not receive any treatment and 2 were only monitored. Systemic corticosteroid therapy was administered to 75 patients, accounting for 63.56% (75/118). Surgical treatment was given to 48 patients, accounting for 40.68% (48/118). It is worth noting that some patients were not initially diagnosed with IgG4-SC before surgery, but with cholangiocarcinoma, PSC, or other bile duct diseases. Out of the 48 patients who received surgical treatment, 16 also received steroid therapy (13.56%, 16/118). Surgical methods were selected based on individual patient conditions. These methods included hepatic lobectomy, cholecystectomy, Whipple (pancreaticoduodenectomy), hepatobiliary jejunostomy, bile duct stent implantation, and Oddi sphincterotomy. Additionally, some patients received anti-tumor drugs and immunosuppressants, as well as anti-infection, choleretic, liver protection, and symptomatic supportive treatments. Approximately two-thirds of the 118 patients mentioned the prognosis, with most recovering well after comprehensive treatment and maintaining an asymptomatic state. However, five patients died due to severe complications, including multiple organ failure and respiratory failure.
Discussion
The study indicates that IgG4-SC patients are predominantly middle-aged and older Asian males. The clinical characteristics observed are jaundice (58.88%), weight loss (22.43%), abdominal pain (20.56%), itchy skin (14.95%), fatigue or weakness (14.02%), dark or dark urine (9.35%), and light stool color (4.67%). Additionally, yellow skin and/or scleral stain were observed in 17% of patients. Its symptoms include painless swelling, abdominal tenderness, elevated serum IgG4 concentration, bile duct stenosis, bile duct dilatation, and biliary wall thickening. Treatment mainly involves steroids, with surgery being necessary for only a few patients. The prognosis for most patients is good.
IgG4-RD was first reported by Japanese scholars in 2001. The disease IgG4-Related Disease (IgG4-RD) is a chronic condition that can affect multiple organs in the body. In addition to the bile duct, IGG4-RD can also affect the pancreas, resulting in autoimmune pancreatitis, pituitaritis, Riedell thyroiditis, retroperitoneal fibrosis, and other conditions. This is characterized by enlargement of the affected organ, which can cause symptoms of obstruction or compression, leading to organ dysfunction. It is important to note that all evaluations presented are objective and free from bias [1].
Igg4-associated sclerosing cholangitis is a manifestation of IGG4-RD biliary tract involvement [2]. It is most commonly observed in elderly men and is characterized by obstructive jaundice with abdominal pain, significantly elevated serum IgG4 levels, segmental or diffuse intrahepatic and/or extrahepatic bile duct stenosis, and bile duct wall infiltration by a large number of IGG4-positive plasma cells and lymphocytes, and extensive fibrosis. Steroid treatment has been found to be effective. IgG4- SC typically presents no clinical symptoms in the early stages of the disease. As the disease progresses, symptoms such as jaundice, abdominal pain, and abnormal liver function may appear. In cases where biliary tract infection is present, fever may also occur. In some cases, IgG4-SC is secondary to autoimmune pancreatitis, which may cause pancreatic enlargement in addition to jaundice and abdominal pain. When combined with other organ damage, corresponding organs may enlarge and/or experience functional impairment. For example, salivary gland and lacrimal gland enlargement, retroperitoneal fibrosis, and renal tubulointerstitial nephritis may occur [3].
Elevated serum IgG4 levels are considered a specific manifestation of IgG4-RD. The diagnosis of IgG4-RD in many patients early in the course of the disease depends on a significant increase in serum IgG4 concentration [4]. Therefore, changes in serum IgG4 levels can be an important diagnostic criterion. According to the 2020 Japanese IgG4-RD Comprehensive Diagnostic (RCD) criteria, a serum IgG4 level >135 mg/dL is helpful for diagnosis. There are a small number of patients who can be pathologically diagnosed with IGG4-RD despite having normal serum IgG4 levels. It is worth noting that an increase in serum IgG4 levels can also be caused by Primary Sclerosing Cholangitis (PSC), Cholangiocarcinoma (CC), and pancreatic cancer, indicating that while the sensitivity of IgG4 level increase is strong, its specificity is poor.
The imaging findings of IgG4-SC patients typically include tube wall thickening and bile duct stenosis. Abdominal Computed Tomography (CT) and magnetic resonance cholangiopancreatography often reveal limited or diffuse bile duct stenosis, proximal bile duct dilatation, uneven diffuse thickening of the bile duct wall, and peribiliary tumorous soft tissue hyperplasia. The affected site is mostly the lower common bile duct [5]. The condition can be classified into four types based on the involved parts. Type I involves stenosis of the lower bile duct, while Type II involves diffused stenosis in both the intrahepatic and extrahepatic bile ducts, which is further subdivided into two subtypes. Type 2a is characterized by intrahepatic bile duct stenosis with prestenotic dilatation. Type 2b shows intrahepatic bile duct stenosis without prestenotic dilatation and reduced bile duct branching, and should be distinguished from PSC’s “pruning tree”-like presentation. Type III involves hilar disease and lower bile duct stenosis. Type IV is characterized by bile duct stenosis present only in hilar lesions [6]. This type is helpful in distinguishing IgG4-SC from PSC, CC, and other diseases. IgG4- SC mainly affects the extrahepatic and intrahepatic bile ducts, causing significant lymphoplasmic infiltration. This results in thickening of the tube walls, fibrosis, and occlusive phlebitis. At the lesion site, significant lymphoplasmic infiltration and fibrosis may be present. The ratio of IGG4-positive plasma cells to IGG-positive cells in each high-power microscope field was greater than 40%, with more than 10 IGG4-positive plasma cells. Typical tissue fibrosis, especially storiform fibrosis and obliterated phlebitis, was also observed [1].
The primary medication currently used for IgG4-SC is steroids, which may have immunosuppressive properties and antiinflammatory effects. The 2019 Clinical Practice Guideline for IgG4-associated sclerosing Cholangitis [7] recommends oral prednisolone at a dose of 0.6 mg/kg/day for initial remission induction therapy. This should be gradually reduced to a maintenance dose of 5 mg/day over 2 to 3 months, which should be sustained for at least 3 years. Steroid use can be discontinued in patients with satisfactory imaging and serological improvement. After stopping treatment, patients should be followed up for recurrence. Most patients respond well to steroid therapy. However, a small number of patients experience relapse or disease progression. Some researchers have also explored the use of methotrexate, azathioprine, cyclophosphamide, rituximab and other drugs, but their effectiveness varies from person to person. Therefore, the efficacy of these drugs in treating this disease is still controversial. Furthermore, some patients with IgG4-SC underwent surgical treatment, which can be divided into two types: focal excision and biliary drainage. It is worth noting that the majority of patients who underwent focal resection were initially misdiagnosed as having cholangiocarcinoma [8]. The main surgical procedures included choledochotomy, Roux-Y anastomosis of the hepatobiliary duct and jejunum, and partial hepatectomy. The postoperative pathological diagnosis for IgG4-SC is often delayed. Regular steroid application can effectively control the disease after diagnosis. Patients with biliary drainage can undergo various operation methods, such as Percutaneous Transhepatic Biliary Drainage (PTCD), laparoscopic T-tube drainage for common bile duct exploration, and biliary stent implantation via ERCP. However, it can only alleviate the symptoms of biliary stasis by draining bile and cannot provide a fundamental solution to the problem of hepatobiliary stenosis.
In summary, steroid therapy is currently the most effective treatment. The effectiveness of immunosuppressants and biological agents in treating this disease is yet to be verified. Surgical treatment may be necessary in cases of severe cholestasis or compression symptoms involving other organs. Improving awareness of IgG4-SC is crucial, and early diagnosis is key to effective treatment.
Declarations
Data availability statement: The original contributions presented in this study are included in this article material, further inquiries can be directed to the corresponding author.
Ethics statement: Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements (Not applicable).
Funding: No fundings.
Competing interest: All authors disclosed no relevant relationships.
References
- Umehara H, Okazaki K, Kawa S, et al. The 2020 Revised Comprehensive Diagnostic (RCD) criteria for IgG4-RD [J]. Mod Rheumatol. 2021; 31(3): 529-533. The DOI: 10.1080/14397595.2020.1859710 IF: 2.2 Q4.
- Kamisawa T, Zen Y, Pillai S, et al. IgG4-related Lancet. 2015; 385(9976): 1460-1471. (in Chinese) DOI:10.1016/S0140-6736(14)60720-0IF: 168.9Q1.
- Maritati F, Peyronel F, Vaglio A. IgG4-related disease: A clinical perspective. Rheumatology (Oxford). 2020; 59: iii123 - iii131. Doi: 10.1093 / rheumatology/kez667IF: 5.5 Q1.
- Yu Jiali, Zhu Lei. Diagnosis and treatment of IGG4-associated sclerosclerosis cholangitis [J]. Journal of Dalian Medical University. 2022; 44(05): 456-465.
- Choi SY, Kim SH, Kang TW, et al. Differentiating mass-forming autoimmune pancreatitis from pancreatic ductal adenocarcinoma on the basis of contrast-enhanced MRI and DWI findings [J]. Am J Roentgenol. 2016; 206(2): 291-300. The DOI: 10.2214 / AJR. 15.14974 IF: 5.0 Q1.
- Chen Ting, Li Sheng, Ru Li. Clinical and imaging observation and literature review of IGG4-associated sclerosing cholangitis of common bile duct [J]. Journal of Medical Imaging. 2019; 29(1): 83-86.
- Kamisawa T, Nakazawa T, Tazuma S, et al. Clinical practice guidelines for IgG4-related sclerosing cholangitis [J]. J Hepatobiliary Pancreat Sci. 2019; 26(1): 9-42. DOI: 10.1002 / JHBP. 596 if: 3.0 Q2.
- Peng Xin, sincere belief. Delayed diagnosis of IGG4-associated sclerosing cholangitis: A case report [J]. Journal of clinical and experimental pathology. 2020; 4 (3): 370-371. The DOI: 10.13315 / j.carol carroll nki cjcep. 2020.03.034.