
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Gall bladder carcinoma masquerading as bouveret syndrome as the initial presentation
Hind El Naamani1*; Adnan Ezici2; Ahmad Al Nawaiseh1; Syed K Mahmood2; Sandeep Krishnan2; Eduardo A Vega3
1Department of Medicine, St. Elizabeth’s Medical Center, Boston, Massachusetts, USA.
2Department of Medicine, Division of Gastroenterology, St. Elizabeth’s Medical Center, Boston, Massachusetts, USA.
3Department of Surgery, Division of Surgery, St. Elizabeth’s Medical Center, Boston, Massachusetts, USA.
*Corresponding Author: Hind El Naamani
Department of Medicine, St. Elizabeth’s Medical Center,
Boston, Massachusetts, USA.
Email: Hind.ElNaamni@steward.org
Received : Apr 19, 2024
Accepted : May 06, 2024
Published : May 16, 2024
Archived : www.jclinmedimages.org
Copyright : © Naamani HE (2024).
Abstract
Introduction: Gallbladder Cancer (GBC) is a rare yet serious condition that often presents diagnostic challenges due to its nonspecific symptoms, which are similar to other biliary disorders. Advanced stages of GBC can lead to rare complications like Cholecystoenteric Fistulas (CEF) or Bouveret Syndrome, where a gallstone migrates and causes Gastric Outlet Obstruction (GOO). We present a case of a woman who presented with symptoms of GOO but later led to the unexpected discovery of GBC.
Case presentation: A 75-year-old female with a history of breast cancer and non-small cell lung cancer treated with surgical resection and radiotherapy presented with abdominal discomfort, postprandial emesis, and weight loss. On examination, vitals were stable. Physical exam notable for abdominal distention with Right Upper Quadrant (RUQ) tenderness. Laboratory tests showed leukocytosis (12.9 x 109 /L), elevated C-Reactive Protein (18 mg/ld.), hypoglycemia (52 mg/dL), decreased albumin (2.3 g/dL). Liver function tests and lipase were within normal range. A Cat scan of the abdomen showed GOO and a possible infiltrating gallbladder lesion. Endoscopy revealed partial GOO at duodenal level. Duodenal biopsy showed peptic injury. Magnetic Resonance Cholangiopancreatography revealed a decompressed gallbladder with inflammation in the gallbladder fossa and around the adjacent pylorus, but no mass causing GOO was found. Instead, a potential stone in the pyloric channel was observed, possibly resulting from erosion from the adjacent gallbladder (suspicion of Bouveret syndrome). After clinical improvement and confirming no fistulous tract with radiology, surgical intervention was not advised, leading to her discharge home. However, she presented 2 weeks later with similar presentation. New CT demonstrated a 3 cm narrowing of the second duodenum and a 13 mm gallstone embedded in the wall of the second part of duodenum. Repeat EGD revealed GOO due to extrinsic compression of the duodenal lumen. Consequently, the patient underwent a open cholecystectomy, gallbladder-duodenal fistula take down, and Billroth 2 gastro-jejunal anastomosis. Intraoperatively, significant findings included a gallbladder-duodenal fistula and adherence of the duodenum to aorto-caval space. Postoperative pathology showed well-differentiated gallbladder adenocarcinoma with perimuscular connective tissue spread. Lymph node involvement could not be determined due to the specimen rupture. Tumor was staged as T3NxM0.
Discussion: GBC is a rare but significant type of cancer, accounting for half of all biliary tract cancers and the fifth most common Gastrointestinal (GI) cancer. Its diagnosis is often delayed due to non-specific symptoms, which can range from none to vague GI complaints like abdominal pain, nausea, and jaundice. An unusual complication of GBC is CEF, it occurs in a small fraction of patients and complicates diagnosis due to its non-specific symptoms. Another rare condition, Bouveret syndrome, involves a migrating gallstone causing an obstruction in the GI tract resulting in GOO. This case presents a patient with GBC manifesting as Bouveret syndrome, highlighting the complexity of diagnosing and managing such cases of concurrent biliary conditions. Despite ongoing surveillance for her known lung cancer with Positron Emission Tomography scan (PET), GBC was not detected until advanced stages, highlighting the difficulties in early detection and the need for vigilance.
Keywords: Bouveret’s syndrome; Cholecystoduodenal fistula; Gallbladder cancer; Gallstone; Gastric outlet obstruction.
Citation: Naamani HE, Ezici A, Nawaiseh AA, Mahmood SK, Krishnan S, et al. Gall bladder carcinoma masquerading as bouveret syndrome as the initial presentation. Open J Clin Med Images. 2024; 4(1): 1184.
Introduction
Gallbladder Cancer (GBC), though uncommon, is a serious medical condition that frequently poses diagnostic challenges [1]. Its non-specific symptoms often mimic those of other biliary disorders, complicating the diagnostic process [1]. In advanced stages, GBC can invade nearby structures, resulting in the formation of Cholecystoenteric Fistulas (CEF). In rare instances, a gallstone may pass through this fistula, leading to an obstruction and subsequent gallstone ileus, causes Gastric Outlet Obstruction (GOO). This specific and rare manifestation of gallstone causing GOO is known as Bouveret Syndrome which is a a rare complication of gallstone disease accounting to only 0.3% to 0.5% of the cases [2]. The combination of GOO, cholecystoenteric fistula, and gallbladder cancer is unusual.
This case report details the diagnostic journey and management of a 75-year-old woman who initially presented with symptoms suggestive of GOO. Her clinical presentation and subsequent investigations provided an intriguing diagnostic puzzle, intertwining symptoms of a common gastrointestinal problem with the complexities of biliary tract pathology. The case is notable for its initial indication towards Bouveret syndrome. However, the situation took an unexpected turn when an Esophagogastroduodenoscopy (EGD) failed to visualize an obstructing stone necessitating a surgical approach. Eventually, she had the discovery of CEF intra-operatively and the eventual diagnosis of gallbladder cancer. This report aims to shed light on the diagnostic challenges and considerations in managing such complex biliary cases, emphasizing the importance of a comprehensive and multi-faceted diagnostic approach.
Case presentation
A 75-year-old female with a history of breast cancer status post-lumpectomy, non-small cell lung cancer treated with right upper lobe wedge resection and radiotherapy in 2017, COPD (chronic obstructive pulmonary disease) and hypertension presented with a 3-week history of abdominal discomfort, postprandial emesis, and 10 lbs weight loss. Upon examination, vital signs were stable. Notable findings included dry mucous membranes and abdominal distention with Right Upper Quadrant (RUQ) tenderness. Laboratory tests showed leukocytosis (12.9 x 109 /L), elevated C-Reactive Protein (18 mg/ld.), hypoglycemia (52 mg/dL), decreased albumin (2.3 g/dL). Liver function tests and lipase were within normal range.
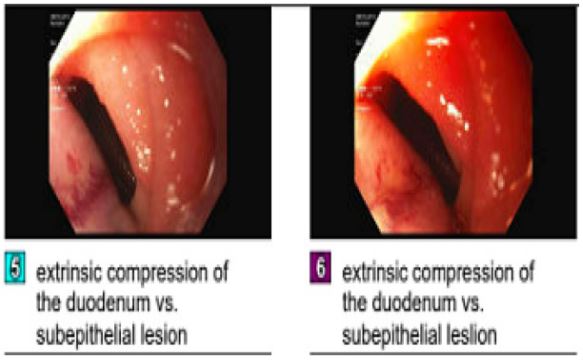
A CT scan of the abdomen showed an enlarged stomach with a large air-fluid level, suggestive of gastric outlet obstruction. The gallbladder was contracted and closely adhered to the liver, indicating a possible infiltrating gallbladder lesion. She was admitted as a case of gastric outlet obstruction. Initially she required NG tube placement. GI performed an endoscopy using an ultrathin scope, as standard equipment was inadequate. The endoscopy revealed a partial gastric outlet obstruction at the duodenal sweep level (Figure 1). A duodenal biopsy indicated peptic injury but no signs of celiac disease, dysplasia, or malignancy. Given the lack of endoscopic evidence explaining her symptoms and the suspicion of a gallbladder lesion, an MRCP (Magnetic Resonance Cholangiopancreatography) was performed. This revealed a decompressed gallbladder with inflammation in the gallbladder fossa and around the adjacent pylorus, but no mass causing gastric outlet obstruction was found. Instead, a potential stone in the pyloric channel was observed, possibly resulting from erosion from the adjacent gallbladder (Bouveret syndrome). Surgical consultation and review with the radiologist did not identify any fistulous tract, so no surgery was recommended at that time. During her hospital stay, the patient began to improve clinically, tolerating a clear liquid diet, which was then progressed to a low-residue diet before she was eventually discharged home.
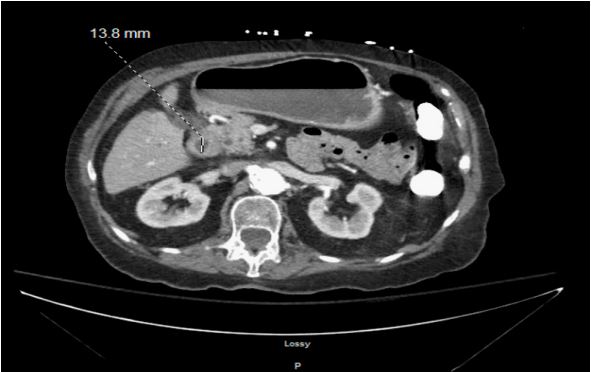
However, she was readmitted 2 weeks later due to ongoing postprandial vomiting and inability to tolerate food. A new CT scan demonstrated a distended stomach with fluid and air, alongside a persistent 3 cm narrowing of the second duodenum (Figure 2). A 13 mm noncalcified gallstone appeared embedded in the wall of the second duodenum, with the adjacent gallbladder appearing decompressed and adherent to segment 4 of the liver (Figure 3). A subsequent repeat EGD revealed food retention in the gastric fundus and the duodenum. A moderate stenosis of the duodenal lumen due to extrinsic compression was noted near the apex of the duodenal bulb, suggesting either a duodenal subepithelial lesion or a large gallstone, potentially indicative of Bouveret’s syndrome. Given her intractable vomiting and the inability to visualize an impacted stone in the pylorus or duodenum during endoscopy this necessitated surgical intervention, both to alleviate the symptoms and to explore the possibility of a fistulous tract. Consequently, the patient underwent an open cholecystectomy, gallbladder-duodenal fistula take down, and Billroth 2 gastro-jejunal anastomosis. Intraoperatively, significant findings included a gallbladder-duodenal fistula and adherence of the duodenum to aortocaval space, raising suspicions of chronic inflammation or neoplastic involvement.
The patient was discharged to a rehabilitation facility with instructions to follow up with her surgeon about her biopsy results. The postoperative pathology of her gallbladder revealed a well-differentiated adenocarcinoma, which had spread to the perimuscular connective tissue. Lymph node involvement and margin status could not be determined due to the specimen being ruptured. The tumor was staged as T3NxM0.
Patient was lost to follow-up and missed her appointment. One month later she presented to the ED with worsening right upper quadrant pain and evidence of cholestatic liver injury. Total bilirubin 8.8 mg/dl, AST 317 U/L, ALT 171 U/L and tumor markers CA 19-9 608 U/ml (Normal <35 U/ml) and CA-125 189 U/ml (normal range 0-35 u/ml). CT Abdomen/Pelvis showed status post cholecystectomy with prominent Inta Hepatic Biliary Duct and Extra Hepatic Biliary Duct biliary dilatation with an abrupt termination of the midportion of common bile duct. For biliary decompression, GI attempted ERCP x3 but due to constriction, they were unsuccessful. On initial ERCP attempt they were unable to reach ampulla as afferent limb was too long. Therefore, entered pylorus and attempted to reach ampulla through strictured duodenal site with AXIOS stent placement/ dilation but on repeat attempt they were still unable to traverse and therefore unable to perform ERCP for biliary decompression. IR were consulted and the patient underwent successfully a percutaneous biliary drainage.

Discussion
Gallbladder Cancer (GBC), while not a common type of cancer, represents nearly half of all cancers found in the biliary tract. It ranks as the fifth most frequent cancer within the gastrointestinal system. The rarity and nonspecific symptoms of GBC often lead to its late diagnosis and thus incidental discovery. Most diagnoses occur during standard cholecystectomy procedures or are identified postoperatively in the final pathology reports intended for other medical reasons [1,3].
The symptoms of Gallbladder (GB) cancer can range significantly, from showing no symptoms at all to exhibiting vague gastrointestinal signs. These may include abdominal pain, nausea, vomiting, indigestion, fatigue, loss of appetite which can resemble cholecystitis. In some cases, there are obstructive symptoms such as jaundice, clay-colored stools, dark urine, and pruritis [1]. In advanced cases it invades adjacent organs by forming Cholecystoenteric Fistula’s (CEF) which accounts for only 3%-14% of cases [4]. CEF is the abnormal connection between the GB and the contiguous organs of the GI tract which is an unusual complication of biliary diseases. CEF occurs in only 3%-5% of patients with cholelithiasis and 0.15%-4.8% of those undergoing biliary surgery. The predominant symptoms associated with Gallbladder Cancer (GBC)-related Cholecystoenteric Fistula (CEF) include abdominal pain (68.8% of cases), nausea or vomiting (62.5%), and weight loss (25%). The non-specific nature of these symptoms, along with the general signs and lab test results, makes the preoperative diagnosis of CEF a challenging task [4].
On the other hand, Bouveret syndrome is when the gallstone travels from the biliary system to the bowel through a biliaryenteric fistula. The stone usually gets impacted either in proximal duodenum or pylorus thus manifesting as gastric outlet obstruction. This phenomenon occurs due to pressure necrosis from gallbladder wall to adjacent organ (bowels) either secondary to acute cholecystitis which occurs in 2-3% of all cases or rarely in the setting of GB malignancy [2]. The combination of cholecystoenteric fistula, gastric outlet obstruction, and gallbladder cancer is unusual. In 2010, Shinoda et al. reported the first case of Bouveret syndrome accompanied by an incidentally discovered gallbladder cancer [5].
In our patient, we encountered a complex interplay of biliary diseases and their complications where GB cancer manifested as Bouveret syndrome as an initial presentation. Clinically, the patient exhibited symptoms of Gastric Outlet Obstruction (GOO) including nausea and postprandial vomiting raising concern of an intrinsic or extrinsic blockage. Later on, imaging showed gastric distention and evidence of a 13 mm noncalcified gallstone embedded in the wall of the second duodenum implicating that a gallstone traveled from the biliary system to the bowel through a biliary-enteric fistula, eventually becoming impacted in the proximal duodenum which eventually led to the manifestations of gastric outlet obstruction. This finding pointed towards the possibility of Bouveret syndrome. However, the inability to visualize an impacted stone in the pylorus or duodenum during endoscopy questioned the diagnosis and necessitated surgical intervention, both to alleviate the symptoms and to explore the fistulous tract further. The patient underwent a series of surgical procedures, including an open gastrostomy, cholecystectomy, closure of a gallbladder-duodenal fistula, and a gastrojejunostomy Billroth II bypass. Pathological examination of the gallbladder later confirmed the presence of a well-differentiated adenocarcinoma with a TNM stage: pT2a.
In this case, the diagnostic and management complexities were significantly heightened due to the diverse range of symptoms and the concurrent occurrence of multiple rare biliary conditions. This patient’s experience with Gallbladder Cancer (GBC) was atypical, emphasizing the importance of considering a wide range of differential diagnoses in such intricate medical cases.
The patient’s medical history adds further layers to this complexity. Notably, she underwent a PET scan in 2022 as part of ongoing surveillance for lung cancer, which showed no abnormal uptake in the gallbladder or bile ducts, indicating no apparent signs of GBC at that time. However, in October 2023, a CT scan of the abdomen and pelvis was done for vague abdominal pain and at that time revealed gallbladder wall thickening and an echogenic focus in the wall of the gallbladder with ring down artifact, suspicious for gallbladder adenomyomatosis. These non-specific findings were not further investigated. Then when she presented in December with the above presentation her CT scan showed only a decompressed gallbladder that is adherent to the adjacent segment 4 of liver. The imaging in her case didn’t show any suspicious of GBC. Computed Tomography (CT) scans are the preferred imaging method for detecting and staging Gallbladder Cancer (GBC) [6]. A retrospective analysis was conducted by George et al on Contrast-Enhanced Computed Tomography (CECT) scan results from cases that were histopathologically confirmed as gallbladder carcinoma. In this study, 49 cases were identified as adenocarcinoma, and one as squamous cell carcinoma. The most common finding was a subhepatic mass, either replacing or obscuring the gallbladder with adjacent liver invasion, observed in (56%) of the cases. This was followed by intraluminal masses in the gallbladder (25%). Least commonly observed, in (24%) cases, was focal or diffuse gallbladder wall thickening. This particular finding poses diagnostic challenges, as gallbladder wall thickening can occur in a variety of clinical situations, including chronic cholecystitis and adenomyomatosis [7]. Similar to our patient where her thickening of GB was not investigated as it was labeled as possible adenomyomatosis. This progression and subtle findings on imaging highlights the inherent challenges in detecting GBC early, as it can evolve and manifest subtly over time.
This case highlights the critical importance of maintaining a high degree of suspicion for Cholecystoenteric Fistula (CEF) as a possible presentation of Gallbladder Cancer (GBC), especially given the often-vague nature of its symptoms. The recognition of CEF as part of the differential diagnosis is vital, particularly because the suspicion of GBC necessitates a different surgical approach. Prior to undertaking an emergency cholecystectomy, it is essential to identify the condition pre-operatively. This approach not only facilitates the planning for an open radical surgery, tailored to address the specific needs of GBC treatment, but also plays a crucial role in minimizing the risk of intraoperative bile spillage [6].
The evolution of the patient’s condition, from no detectable signs on PET scan to identifiable changes on CT scan that are non-specific and within a relatively short period, illustrates the deceptive nature of GBC and the critical need for ongoing, comprehensive evaluation in patients with complex medical histories. This case serves as a reminder of the dynamic and often unpredictable nature of cancer progression and the need for adaptability in diagnostic and treatment strategies in oncology.
References
- Mukkamalla SKR, Kashyap S, Recio-Boiles A, et al. Gallbladder Cancer. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024. https://www.ncbi.nlm.nih.gov/books/NBK442002/#
- Turner AR, Kudaravalli P, Al-Musawi JH, et al. Bouveret Syndrome (Bilioduodenal Fistula). In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024. https://www.ncbi.nlm.nih.gov/books/NBK430738/
- Shaffer EA. Gallbladder cancer: The basics. Gastroenterol Hepatol (N Y). 2008; 4(10): 737-41.
- Wang CY, Chiu SH, Chang WC, Ho MH, Chang PY. Cholecystoenteric fistula in a patient with advanced gallbladder cancer: A case report and review of literature. World J Clin Cases. 2023; 11(36): 8519-8526
- Shinoda M, Aiura K, Yamagishi Y, Masugi Y, Takano K, et al. Bouveret’s syndrome with a concomitant incidental T1 gallbladder cancer. Clin J Gastroenterol. 2010; 3(5): 248-53.
- Ramachandran A, Srivastava DN, Madhusudhan KS. Gallbladder cancer revisited: the evolving role of a radiologist. Br J Radiol. 2021; 94(1117): 20200726.
- George RA, Godara SC, Dhagat P, Som PP. Computed Tomographic Findings in 50 Cases of Gall Bladder Carcinoma. Med J Armed Forces India. 2007; 63(3): 215-9.
- Turner AR, Kudaravalli P, Al-Musawi JH, Ahmad H. Bouveret syndrome (bilioduodenal fistula). 2017.