
Open Journal of
Clinical and Medical Images
Review Article - Open Access, Volume 4
Harnessing the power of clinical data in dentistry: Importance and guidelines for dentists in AI modelling for enhanced patient care
Seyed-Ali Sadegh-Zadeh1*; Mahshid Bagheri2
1Department of Computing, School of Digital, Technologies and Arts, Staffordshire University, Stoke-on-Trent, ST4 2DE, UK.
2Faculty of Dentistry, Oral & Craniofacial Sciences, King’s College London, London, UK.
*Corresponding Author: Seyed-Ali Sadegh-Zadeh
Department of Computing, School of Digital, Technologies and Arts, Staffordshire University, Stoke-on-Trent,
ST4 2DE, UK.
Email: ali.sadegh-zadeh@staffs.ac.uk
Received : Apr 26, 2024
Accepted : May 31, 2024
Published : Jun 07, 2024
Archived : www.jclinmedimages.org
Copyright : © Sadegh-Zadeh SA (2024).
Abstract
Objectives: This paper aims to explore the significance of clinical data in the integration of AI technologies into dentistry, highlighting its role in enhancing diagnostic accuracy, treatment planning, and patient care. It also provides guidelines for dentists to effectively harness clinical data for improved dental healthcare.
Data: The data discussed in this paper comprises patient records, radiographs, intraoral scans, and treatment outcomes, all of which are essential components for AI-driven dentistry.
Sources: The primary sources of data include clinical records and related information generated in dental practices. The paper also draws from the broader field of artificial intelligence in healthcare.
Study selection: The study selection involves a comprehensive examination of existing research, case studies, and practical insights related to the integration of AI and clinical data in dentistry.
Conclusion: This paper underscores the critical role of quality clinical data in successfully implementing AI models in dentistry. It empowers dental practitioners with the knowledge and guidelines necessary to harness the transformative potential of AI-driven dentistry, leading to improved diagnostic precision, personalized treatment strategies, and enhanced patient experiences. The paper addresses data collection, preprocessing, challenges, ethical considerations, and future directions of AI in dentistry, providing dentists with the tools to advance dental care through clinical data-driven AI.
Keywords: Clinical data; AI modelling; Patient care; Data collection; Data privacy; Data standardization.
Citation: Sadegh-Zadeh SA, Bagheri M. Harnessing the power of clinical data in dentistry: Importance and guidelines for dentists in AI modelling for enhanced patient care. Open J Clin Med Images. 2024; 4(1): 1188.
Introduction
Advancements in Artificial Intelligence (AI) have ushered in a new era of healthcare, promising enhanced diagnostic accuracy, treatment planning, and patient care [1]. Dentistry, as a vital component of healthcare, stands to benefit significantly from the integration of AI technologies. One of the key driving factors behind the success of AI in dentistry is the availability and utilization of clinical data. This paper aims to delve into the importance of clinical data in dentistry’s AI modelling and provide guidelines for dentists to harness this data effectively for improved patient care.
The field of dentistry has evolved beyond traditional practices and now incorporates cutting-edge technologies to diagnose and treat oral health issues [2]. AI, particularly machine learning, has demonstrated remarkable potential in interpreting complex clinical data, aiding in early disease detection, treatment planning, and decision-making. Clinical data, encompassing patient records, radiographs, intraoral scans, and treatment outcomes, hold a wealth of information that AI algorithms can leverage to enhance accuracy, efficiency, and patient outcomes [3]. However, realizing the full potential of AI in dentistry necessitates a comprehensive understanding of how to collect, preprocess, and apply clinical data effectively.
The primary objective of this paper is to underscore the pivotal role of clinical data in the successful implementation of AI models within dentistry. By emphasizing the importance of quality clinical data, we seek to empower dentists with the knowledge and guidelines required to contribute to the development and application of AI technologies. This paper will elucidate the multifaceted benefits that AI-driven dentistry offers, including improved diagnostic precision, personalized treatment strategies, and enhanced patient experiences.
Clinical data, encompassing a range of patient information such as medical history, radiographic images, dental charting, and treatment outcomes, forms the cornerstone of evidencebased dentistry [4]. The integration of AI within the dental field hinges upon the availability of high-quality, diverse, and representative clinical data. Such data facilitate the training and validation of AI algorithms, enabling them to recognize intricate patterns, correlations, and anomalies that might elude human perception. The significance of clinical data is not confined to its sheer volume but extends to its diversity, as a broader representation of cases ensures generalizability and robustness of AI models [5].
Dentistry has witnessed a surge in digitalization, leading to the accumulation of vast amounts of clinical data in electronic health records, dental imaging systems, and treatment planning software. Leveraging this data effectively can lead to breakthroughs in early disease detection, treatment customization, and prognostic evaluation. Furthermore, the integration of AI can expedite the analysis of radiographs, aid in the identification of pathological conditions, and facilitate the prediction of treatment outcomes, thereby streamlining workflows and elevating the overall standard of patient care [6].
In subsequent sections of this paper, we will delve deeper into the methodologies for harnessing clinical data, outline the challenges associated with its utilization in AI modelling, and provide practical guidelines for dentists to optimize data collection, preprocessing, and integration within AI frameworks. Through this exploration, we aim to equip dental practitioners with the tools and insights needed to unlock the transformative potential of clinical data-driven AI in dentistry.
Type of study
In the realm of harnessing clinical data for AI modelling in dentistry, selecting an appropriate study type is paramount to ensure the reliability and validity of the results [7]. Two fundamental dimensions to consider are the nature of the data collection process and the methods of data analysis [8]. This section delves into two crucial aspects of study design: retrospective vs prospective studies, and qualitative vs quantitative approaches.
Retrospective vs Prospective studies
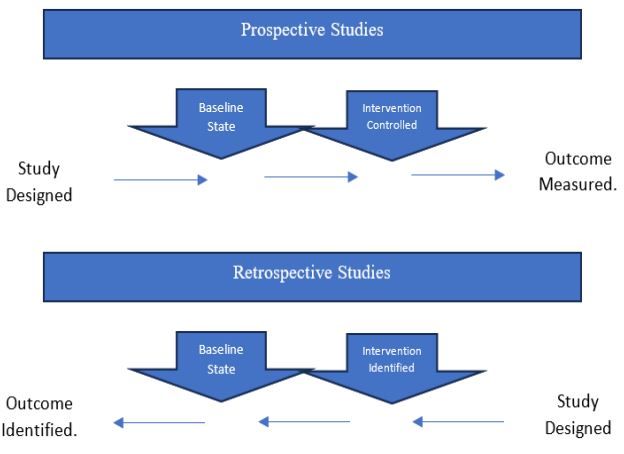
Retrospective and prospective studies are distinct approaches to gathering and analysing clinical data, each offering unique advantages and limitations [9]. The choice between the two depends on the research objectives, available resources, and the specific dental question under investigation.
Retrospective studies involve analysing historical data that have been previously collected for other purposes. In the context of dentistry, retrospective studies can leverage electronic health records, patient charts, and imaging databases to glean insights into patterns, treatment outcomes, and disease progression [10]. These studies are often cost-effective and less time-consuming since the data already exist. However, they are susceptible to biases, missing data, and limited control over data quality [11]. Despite these limitations, retrospective studies can provide valuable preliminary findings that guide the development of more controlled prospective investigations.
Prospective studies, on the other hand, involve the collection of new data from a defined patient cohort over a specific time period. These studies allow for greater control over data quality and can provide stronger evidence for causal relationships between variables [12]. In the context of AI modelling for dentistry, prospective studies can be designed to follow patients undergoing specific treatments or interventions, tracking their progress, outcomes, and potential complications. While prospective studies are generally more resource-intensive and time-consuming, their robust design lends credibility to the results, making them essential for establishing clinical guidelines and improving patient care. Figure 1 represents distinguishing between prospective and retrospective study designs.
Qualitative vs Quantitative approaches
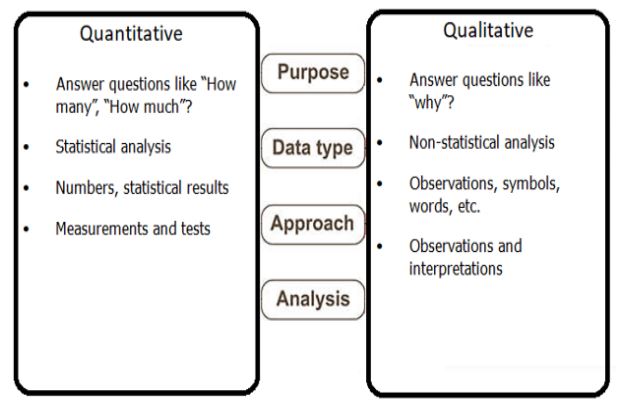
Another pivotal decision in clinical data utilization for AI modelling lies in the choice between qualitative and quantitative approaches to data analysis. These approaches offer complementary perspectives on clinical phenomena, enabling a comprehensive understanding of patient care dynamics.
Qualitative analysis involves exploring the underlying meanings, experiences, and perceptions of patients, dentists, and other stakeholders. Techniques such as interviews, focus groups, and content analysis can uncover nuances that quantitative methods may overlook [13]. In dentistry, qualitative research can unearth patient preferences, barriers to treatment adherence, and contextual factors influencing oral health practices. Integrating qualitative findings into AI models can enhance their accuracy and relevance by accounting for the human element in patient care [14].
Quantitative analysis, on the other hand, focuses on numerical data and statistical relationships. This approach is essential for assessing the effectiveness of treatments, identifying trends in disease prevalence, and quantifying risk factors [15]. By leveraging large datasets of clinical measurements, diagnostic images, and patient demographics, quantitative approaches facilitate the development of predictive models that aid in diagnosis, treatment planning, and patient management [16]. Advanced statistical techniques, such as machine learning algorithms, can extract intricate patterns from these data sources, enabling dentists to make evidence-based decisions [17].
The selection of study type and data analysis approach is pivotal when harnessing clinical data for AI modelling in dentistry. The choice should align with the research objectives, available resources, and the level of evidence required for informed clinical decision-making. Integrating both retrospective and prospective studies, as well as qualitative and quantitative analyses, can yield a comprehensive understanding of dental practices, ultimately leading to enhanced patient care.
The role of clinical data in AI modelling
In recent years, AI has emerged as a transformative technology with the potential to revolutionize various fields of healthcare, including dentistry. The integration of AI techniques within dental practices holds great promise for enhancing patient care, diagnosis, treatment planning, and overall practice efficiency. A critical component of successful AI implementation in dentistry is the utilization of high-quality clinical data. This section delves into the significance of clinical data in AI modelling within the dental domain.
Understanding AI in dentistry
AI, broadly defined as the simulation of human intelligence processes by machines, encompasses a range of techniques such as machine learning, deep learning, and natural language processing [18]. In dentistry, AI can be leveraged to analyse vast amounts of clinical data, identify patterns, make predictions, and offer valuable insights that can aid dentists in making informed decisions. From image analysis of radiographs to datadriven treatment planning, AI has the potential to augment the capabilities of dental professionals, leading to more accurate diagnoses and personalized treatment strategies [19].
Importance of high-quality datasets for AI models
Central to the success of AI models in dentistry is the availability of high-quality clinical datasets. Clinical data, comprising patient records, radiographic images, treatment histories, and other relevant information, serve as the foundation upon which AI algorithms are built and refined. The quality of these datasets significantly influences the performance and reliability of AI models [20]. Well-curated and comprehensive datasets ensure that AI algorithms are trained on diverse cases, leading to robust models capable of handling a variety of patient scenarios.
Dentists play a crucial role in curating and preparing these datasets. Accurate and standardized data collection, including patient demographics, medical history, dental charts, and treatment outcomes, is essential to ensure the integrity of the dataset. Dentists must also collaborate with data scientists to address issues related to data privacy, security, and compliance with regulations such as HIPAA and GDPR safeguarding patient confidentiality while maximizing the potential of AI modelling. HIPAA (Health Insurance Portability and Accountability Act) regulations protect the privacy and security of individuals’ health information [21]. The General Data Protection Regulation (GDPR) is a comprehensive European Union (EU) law that aims to protect the privacy and data rights of individuals by regulating the collection and processing of their personal data by organizations [22].
Data analytics lifecycle model
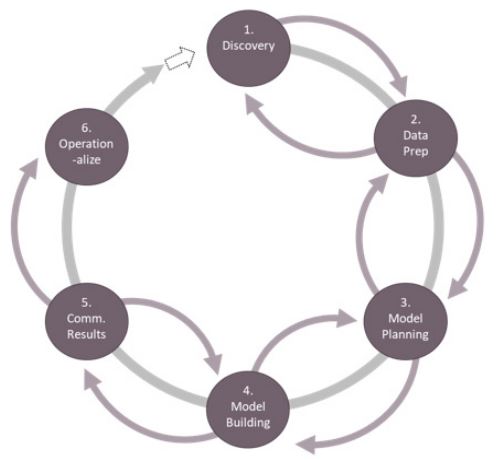
Figure 3 shows the data analytics lifecycle model, which comprises six crucial stages that collectively drive effective data-driven decision-making. It all begins with Discovery, where businesses gain an understanding of their objectives, align resources, and lay the foundation for a successful data analytics project. Following this is the Data Preparation stage, where raw data is cleaned, transformed, and made ready for analysis. In Model Planning, analysts strategize their approach to solving the problem, choosing appropriate techniques and tools. Model Building is the phase where algorithms are applied to the prepared data, creating predictive or descriptive models. Once these models are generated, it’s time to Communicate Results, conveying findings to stakeholders in a comprehensible manner. Lastly, operationalize ensures that the models are integrated into the organization’s processes, enabling ongoing datadriven decision-making [23,24]. This lifecycle model serves as a roadmap for organizations seeking to harness the power of data analytics effectively.
Benefits of AI applications in dentistry
The application of AI in dentistry brings forth a myriad of benefits that have the potential to transform patient care and practice management. One of the most significant advantages is the ability to expedite diagnosis and treatment planning [25]. AI models trained on large datasets can rapidly identify subtle patterns indicative of dental conditions, enabling early detection and intervention. This leads to timely treatments, potentially preventing the progression of diseases and reducing patient discomfort [26].
Furthermore, AI can assist dentists in making more accurate and personalized treatment recommendations. By analysing patient-specific data, such as medical history, oral health records, and genetic factors, AI algorithms can generate tailored treatment plans that align with individual patient needs [27]. This personalized approach enhances treatment outcomes and patient satisfaction. In addition to clinical applications, AI can enhance practice efficiency by automating routine administrative tasks, optimizing appointment scheduling, and improving resource allocation. This streamlining of administrative processes allows dental professionals to focus more on patient interactions and complex cases.
The integration of AI in dentistry has the potential to reshape how dental care is delivered. However, the success of AI modelling hinges upon the quality of clinical data used to train and validate these models. Dentists, as custodians of patient data, play a pivotal role in providing high-quality datasets and collaborating with data scientists to ensure the ethical and effective implementation of AI technologies for enhanced patient care.
Challenges and ethical considerations
As the integration of AI in dentistry becomes more prevalent, dentists and researchers must confront various challenges and ethical considerations associated with utilizing clinical data for AI modelling to enhance patient care [28]. These challenges encompass issues related to data privacy, security, and compliance, as well as the need for de-identification techniques to ensure patient confidentiality. Addressing these concerns is paramount to maintaining patient trust and the responsible development of AI-driven solutions in the dental field [29,30].
Data privacy and patient confidentiality
The principle of patient confidentiality has long been upheld in medical practice, and its significance extends to the realm of AI modelling in dentistry. Clinical data, often containing sensitive patient information, is central to AI development but must be handled with utmost care to preserve patient privacy. Dentists and researchers must be cognizant of data sharing practices and the potential risks of re-identification, where seemingly anonymized data can be traced back to individuals. Proper measures, such as data encryption, access controls, and data minimization, must be employed to safeguard patient information and ensure compliance with privacy regulations [29,31].
Data security and compliance with regulations
Data breaches and unauthorized access pose significant threats to patient data security. As dentists and researchers harness clinical data for AI modelling, adherence to relevant data protection regulations is imperative. Regulations such as the HIPAA in the United States and GDPR in the European Union set stringent requirements for handling and processing healthcare data. Dentists engaged in AI development must be well-versed in these regulations, implement robust security measures, conduct regular risk assessments, and stay updated with evolving cybersecurity best practices to prevent breaches and ensure compliance [29,32].
De-identification techniques for anonymization
To strike a balance between data utilization and patient privacy, de-identification techniques play a pivotal role. De-identification involves removing or altering patient identifiers from clinical data to render them anonymous. This process ensures that the data used for AI modelling cannot be linked back to specific individuals [32-34]. Techniques like pseudonymization, tokenization, and generalization can be employed to effectively anonymize data while retaining its utility for research and AI development [35]. Dentists must acquire a comprehensive understanding of these techniques and integrate them into their AI modelling workflows to mitigate the risks associated with data re-identification.
As the dental field embraces AI modelling to enhance patient care, dentists and researchers must navigate a complex landscape of challenges and ethical considerations. Data privacy, security, and compliance with regulations are crucial aspects that demand meticulous attention. De-identification techniques provide a means to ensure patient confidentiality while enabling meaningful AI-driven insights. By adopting responsible practices and staying abreast of evolving ethical and regulatory standards, dentists can harness the power of clinical data in AI modelling while upholding the highest standards of patient care and privacy.
Collecting and curating clinical data
Effective utilization of clinical data in dentistry requires careful collection and curation of diverse datasets. This section focuses on the key steps involved in identifying relevant data types, selecting appropriate variables, and employing various data collection methods.
Table 1: Data category and advice on how to record. prioritize patient privacy and data security throughout the dataset creation process and comply with relevant regulations, such as HIPAA. Proper documentation, standardized formats, and metadata are essential for creating a valuable and organized dental dataset for research and practice management purposes.
| Data Category | Advice for Recording Data |
|---|---|
| Patient Information | - Collect patient's name, age, gender, and contact information. |
| - Maintain a standardized format for contact info (e.g., phone, email). | |
| - Protect patient privacy and comply with data protection regulations. | |
| Medical History | - Document detailed medical histories, including pre-existing conditions. |
| - Record relevant dates and updates over time. | |
| Dental History | - Gather information on past dental treatments and issues. |
| - Record dates of significant dental events. | |
| Allergies and Medications | - Document known allergies and current medications. |
| Clinical Data | - Store intraoral and extraoral photographs with clear metadata. |
| - Categorize radiographic images (X-rays, CBCT scans) by type and date. | |
| - Organize intraoral scans with information on the scanner used. | |
| - Maintain clinical examination findings in a structured format. | |
| Treatment Records | - Create structured treatment plans with proposed procedures. |
| - Use standardized procedure codes and descriptions. | |
| - Document records of dental procedures performed with dates. | |
| - Store prescription records with medication details. | |
| Radiographic Data | - Categorize radiographic images by type (e.g., bitewing, panoramic). |
| - Include metadata like exposure settings and patient ID. | |
| Laboratory Data | - Record dental impressions and casts with patient identifiers. |
| - Store shade and color matching records with descriptions. | |
| Periodontal Data | - Maintain periodontal charting data with measurement details. |
| - Keep gingival health records and plaque/calculus assessments. | |
| Orthodontic Data | - Organize orthodontic records by type (X-rays, models, photos). |
| - Record bite registrations and appliance placement details. | |
| Endodontic Data | - Document records of root canal treatments with dates. |
| - Store radiographic images of root canals with metadata. | |
| Oral Surgery Data | - Include surgical reports and pre/postoperative records. |
| - Organize records of extractions and other surgical procedures. | |
| Prosthodontic Data | - Record details of crown, bridge, and denture work. |
| - Include information about materials used and fabrication dates. | |
| Dental Laboratory Data | - Maintain work orders for prosthetic fabrication. |
| - Include quality control data for lab work. | |
| Research Data | - Categorize data from clinical trials and studies. |
| - Document research on dental materials and techniques. | |
| Billing and Insurance Data | - Keep records of billing, insurance claims, and payments. |
| - Ensure compliance with healthcare billing regulations. | |
| Practice Management Data | - Record scheduling and appointment data with timestamps. |
| - Keep patient communications and financial records organized. | |
| Patient Consent Forms | - Maintain informed consent forms for various procedures. |
| - Link consent forms to relevant patient records. | |
| Infection Control and Sterilization Data | - Record sterilization cycles for instruments and equipment. |
| - Maintain infection control protocols and compliance records. | |
| Digital Records | - Store electronic health records (EHRs) securely. |
| - Organize digital radiographs and images with clear metadata. | |
| - Keep electronic communication and correspondence records. |
Identifying relevant data types and variables
Dentistry encompasses a wide range of patient-related information that can be valuable for AI modelling. Identifying the right data types and variables is essential to ensure the accuracy and applicability of AI-driven solutions. Commonly considered data types and variables include [36,37]:
a) Patient demographics: Age, gender, ethnicity, and socioeconomic status.
b) Medical history: Existing health conditions, allergies, medications, and relevant medical procedures.
c) Dental history: Previous treatments, surgeries, dental conditions, and oral hygiene practices.
d) Clinical assessments: Examination findings, diagnostic codes, and treatment plans.
e) Radiographic and imaging data: X-rays, intraoral and extraoral images, and 3D scans.
f) Clinical notes and reports: Progress notes, operative reports, and referrals.
g) Treatment outcomes: Post-treatment evaluations, patient satisfaction scores, and complications.
h) Patient surveys and questionnaires: Feedback on pain levels, treatment preferences, and quality of life impact.
Creating a well-structured dataset in dentistry requires careful organization of the information you’ve provided. Table 1 outlines each data category and provides advice on how to record them for creating a comprehensive dental dataset in the future.
Data collection methods
Several data collection methods are commonly employed in dentistry to obtain the necessary information for AI modelling. Each method has its own advantages and challenges.
Electronic Health Records (EHRs)
Electronic Health Records (EHRs) have become central to modern healthcare systems. In dentistry, EHRs store patient demographic details, medical and dental histories, radiographic images, treatment plans, and progress notes [38]. Dentists can tap into EHRs to access comprehensive patient data, fostering a holistic approach to treatment planning. However, challenges may arise due to variations in EHR systems, data quality, and interoperability issues [39,40].
Imaging and radiographic data
Dental imaging, including X-rays, Cone-Beam Computed Tomography (CBCT) scans, and intraoral and extraoral photographs, provides valuable insights for diagnosis and treatment planning [41]. These images offer visual evidence of dental conditions, aiding AI models in accurate diagnosis. Proper storage, retrieval, and integration of imaging data are essential, along with considerations for patient privacy and radiation exposure.
Clinical notes and reports
Clinical notes and reports document patient interactions, treatment plans, and outcomes. These narratives can provide context to quantitative data, enhancing the understanding of patient cases. Structured and standardized documentation practices facilitate data extraction for AI models, but the challenge lies in reconciling diverse formats and terminology [42].
Patient surveys and questionnaires
Patient surveys and questionnaires offer subjective insights into patient experiences, preferences, and outcomes. They can help personalize treatment plans and improve patient satisfaction. Designing effective surveys and ensuring high response rates are crucial to obtaining meaningful data. However, potential biases and the need for careful interpretation should be considered [43].
Collecting and curating clinical data in dentistry involves identifying relevant data types, selecting appropriate variables, and employing diverse data collection methods [44]. Each method comes with its own considerations and challenges, requiring dentists to adopt a strategic and multidimensional approach to harnessing the power of clinical data for AI modelling and enhanced patient care.
Ensuring data quality and accuracy
Data quality and accuracy are paramount when harnessing clinical data for AI modelling in dentistry. Ensuring that the data used to train and validate AI algorithms are reliable and error-free is essential for the success of any AI-driven initiative in healthcare.
Data cleaning and preprocessing
Data cleaning and preprocessing are critical steps in the journey toward high-quality clinical data. Dentists and researchers must follow meticulous procedures to clean and prepare the data before feeding it into AI models. The following techniques can aid in this process [45]:
a) Outlier detection and handling: Identifying and addressing outliers is crucial as they can skew the results and lead to incorrect predictions. Dentists should use statistical methods and visualization techniques to detect outliers and make informed decisions about whether to remove or adjust them.
b) Normalization and standardization: Data often come in various formats and units. Normalization and standardization techniques help bring data to a common scale, making it easier for AI models to interpret and learn from the information. This step ensures that data from different sources can be effectively integrated.
c) Feature engineering: Feature engineering involves selecting, creating, or transforming variables to improve the performance of AI models. Dentists should collaborate with data scientists to identify relevant features and engineer them to enhance the model’s predictive power
d) Handling imbalanced data: In some cases, clinical data may be imbalanced, meaning there are significantly more samples from one class than another (e.g., rare diseases). Dentists should explore techniques like over-sampling, under-sampling, or synthetic data generation to address this imbalance and prevent model bias.
e) Data validation: Cross-validation and validation sets are essential to evaluate the performance of AI models and ensure they generalize well to new data. Dentists should partition their data appropriately and establish rigorous validation protocols.
Dealing with missing data
Missing data is a common challenge in clinical datasets and can negatively impact AI model performance. Dentists need to employ strategies to handle missing data effectively [46]:
a) Data imputation: Dentists can use data imputation techniques to fill in missing values with estimated or predicted values. Imputation methods can include mean imputation, median imputation, or more advanced techniques like regression imputation based on other correlated variables.
a) Assessing the impact: Dentists should assess the impact of missing data on the research or clinical question at hand. Depending on the extent and nature of missingness, they may decide to exclude certain variables or samples from the analysis.
a) Multiple imputation: Multiple imputation is a sophisticated technique that generates multiple datasets with imputed values, accounting for uncertainty. Dentists can use this approach to provide more robust and reliable results.
a) Transparent reporting: When presenting research findings or clinical decisions based on AI models, it is crucial to transparently report how missing data were handled. This ensures the credibility and reproducibility of the study.
Ensuring data quality and accuracy through data cleaning and preprocessing is essential in AI modelling for dentistry. Dentists and researchers should pay close attention to data preparation techniques, handle outliers, normalize data, engineer relevant features, address imbalanced datasets, and develop strategies for handling missing data. These steps contribute to the reliability and robustness of AI models in clinical practice.
Building comprehensive and diverse datasets
To harness the power of clinical data effectively in AI modelling for dentistry, it is essential to build comprehensive and diverse datasets. This section discusses strategies for data sampling, population representation, collaboration with multiple practices or institutions, and the role of multicentre studies in achieving these goals.
Data sampling and population representation
Sampling strategies
Sampling is a critical step in dataset construction. Dentists and researchers must carefully select samples that accurately represent the population of interest. Consider the following sampling strategies [47,48]:
a) Random sampling: Randomly selecting patient data from a larger pool ensures that each case has an equal chance of inclusion. This method reduces selection bias and enhances the dataset’s representativeness.
a) Stratified sampling: Stratification involves dividing the population into subgroups based on specific criteria, such as age, gender, or dental condition. Samples are then randomly selected from each subgroup to ensure representation across all categories.
a) Oversampling underrepresented groups: To address disparities in data representation, consider oversampling underrepresented groups, such as rare dental conditions or demographic minorities. This helps avoid bias and ensures inclusivity.
a) Longitudinal data: Collect data over time to capture changes in patient conditions and treatment outcomes. Longitudinal data provide valuable insights into disease progression and treatment effectiveness.
Ensuring diversity
Diversity within the dataset is crucial to train AI models that can generalize well to various patient populations [49]. Dentists should strive to include data from patients of different age groups, genders, ethnicities, and socio-economic backgrounds. This diversity enhances the model’s ability to adapt to the unique characteristics of individual patients and improves its overall accuracy.
Collaborating with multiple practices or institutions
Collaboration with multiple dental practices or institutions can significantly enrich the dataset used for AI modelling. Dentists should consider the following approaches [50,51]:
a) Data sharing agreements: Establish clear data sharing agreements and protocols with other dental practices or institutions. Ensure compliance with data privacy regulations, and define roles and responsibilities for data collection, management, and sharing.
a) Data standardization: Standardize data collection procedures and terminologies across collaborating practices to ensure data consistency. This step is essential for combining data effectively and reducing variability.
a) Data integration: Develop systems or platforms for seamless data integration from multiple sources. This integration facilitates the creation of a more comprehensive dataset by combining data from various dental practices or institutions.
a) Quality control: Implement quality control measures to verify the accuracy and completeness of data received from collaborators. Regular audits and data validation processes help maintain data integrity.
The role of multicentre studies
Multicentre studies are research investigations conducted at multiple healthcare or research facilities to collect data from diverse populations, enhancing the generalizability of findings. Multicentre studies play a pivotal role in creating diverse and robust datasets for AI modelling in dentistry. These studies involve data collection from multiple dental institutions or clinics, often across different geographic locations. Here are some key considerations for conducting multicentre studies [52]:
a) Study design: Collaborate with participating centres to design a study protocol that addresses specific research objectives. Ensure consistency in data collection methods and criteria for patient inclusion.
a) Data harmonization: Harmonize data collection procedures and variables across all participating centres to ensure uniformity. This step is crucial for combining data effectively and minimizing variability.
a) Ethical approval: Seek ethical approval and clearance from the relevant Institutional Review Boards (IRBs) or ethics committees at each participating centre. Compliance with ethical standards is essential when conducting multicentre studies.
a) Data sharing and governance: Establish data sharing and governance mechanisms to protect patient privacy, comply with regulations, and outline data access policies. Clearly define roles and responsibilities of each centre regarding data management and sharing.
a) Data analysis: Collaboratively analyse the combined dataset to derive meaningful insights. AI models trained on multicentre data can offer a broader perspective on dental conditions and treatment outcomes.
Building comprehensive and diverse datasets for AI modelling in dentistry requires careful consideration of data sampling strategies, population representation, collaboration with multiple practices or institutions, and the implementation of multicentre studies. Dentists, researchers, and institutions should work together to create high-quality datasets that can drive the development of effective AI-driven solutions for enhanced patient care in dentistry.
Data standardization and interoperability
Clinical data standardization and interoperability are critical components of harnessing the power of clinical data in dentistry for AI modelling. Standardization ensures that data collected from various sources are structured in a consistent and uniform manner, while interoperability enables seamless data exchange and integration between different systems and healthcare providers [53,54]. This section discusses the importance of adopting common data standards and ensuring data interoperability for AI models in dentistry.
Adopting common data standards
Dental terminology standardization: Standardizing dental terminology is essential to ensure that data across different dental practices and institutions are described consistently [55]. Common dental coding systems, such as the Current Dental Terminology (CDT) codes [56], facilitate the recording and exchange of dental procedures and diagnoses. Dentists should use standardized coding systems when documenting patient information to promote data uniformity.
Health Information Exchange (HIE) standards: Health Information Exchange (HIE) standards are a set of protocols and formats that enable the secure and interoperable sharing of electronic health information among healthcare organizations and systems [57]. HIE standards play a vital role in enabling the secure and standardized sharing of patient data across healthcare organizations. Dentists should be aware of HIE standards and protocols, such as Health Level Seven International (HL7) [58], to facilitate data exchange between dental practices, hospitals, and other healthcare entities. This interoperability ensures that AI models can access comprehensive patient records for more accurate analysis.
Dental imaging standards: Standardization in dental imaging is crucial for AI models that rely on radiographs and other imaging data. The Digital Imaging and Communications in Medicine (DICOM) standard is a widely used format for storing and transmitting medical images and associated information in a standardized manner [59]. Dentists should ensure that their imaging equipment and software adhere to DICOM standards to enhance data quality and interoperability.
Ensuring data interoperability for AI models
Integration with Electronic Health Records (EHRs): To maximize the utility of clinical data for AI modelling, dentists should work toward integrating AI solutions with existing EHR systems. This integration allows AI models to access real-time patient data and historical records, facilitating more accurate and personalized treatment recommendations [60]. Dentists should collaborate with EHR vendors and IT professionals to ensure seamless integration while maintaining data security.
Cross-platform compatibility: AI models used in dentistry should be designed to run on different computing platforms and operating systems. Ensuring cross-platform compatibility allows dental practices with varying technology infrastructures to adopt AI solutions without compatibility issues [61]. Dentists should select AI software and tools that are adaptable to different environments and technologies.
Data exchange protocols: Implementing standardized data exchange protocols, such as Fast Healthcare Interoperability Resources (FHIR) for healthcare data, enables the efficient and secure sharing of clinical data between systems. FHIR is a standardized framework for exchanging healthcare information electronically, designed to facilitate interoperability in the healthcare industry [62]. Dentists should be familiar with these protocols and ensure that AI models can communicate seamlessly with EHRs, imaging systems, and other data sources. This interoperability enhances the accuracy and timeliness of AIdriven insights.
Data security and privacy
While promoting data interoperability, dentists must prioritize data security and patient privacy. Implementing robust security measures, encryption techniques, and access controls is essential to protect patient information during data exchange [63]. Dentists should also stay updated on data protection regulations and compliance requirements to ensure that AI models adhere to ethical and legal standards.
Data standardization and interoperability are fundamental aspects of leveraging clinical data for AI modelling in dentistry. Dentists should adopt common data standards, facilitate data exchange, and prioritize data security to enable AI models to access, analyse, and utilize clinical data effectively. These efforts not only enhance patient care but also contribute to the responsible and ethical implementation of AI technologies in the dental field.
Data sharing and collaboration
Data sharing and collaboration are essential components of harnessing the power of clinical data in dentistry for AI modelling and enhanced patient care. In this section, we explore the value of open data sharing, the importance of collaborating with researchers and scientists, and strategies to overcome barriers to data sharing.
The value of open data sharing
Open data refers to publicly accessible data that can be freely used, shared, and redistributed by anyone without restrictions or limitations [64]. Open data sharing in dentistry involves making clinical datasets and research findings accessible to a broader community of researchers, practitioners, and data scientists. This approach offers several significant benefits [65,66]:
a) Accelerated research: Open data sharing accelerates the pace of research by allowing multiple teams to work on diverse datasets. This collaborative effort can lead to quicker advancements in AI models, resulting in improved patient care.
a) Diverse perspectives: Sharing data with a wider audience brings in diverse perspectives and expertise. Researchers from various backgrounds can contribute insights and innovative approaches to AI modelling, leading to more robust and accurate algorithms.
a) Validation and reproducibility: Open data sharing facilitates the validation and reproducibility of research findings. Other researchers can independently assess and verify the results, enhancing the credibility of AI models and research outcomes.
a) Data pooling: Combining datasets from multiple sources can lead to larger, more comprehensive datasets. This pooling of data can improve the generalizability and effectiveness of AI models, especially in rare or complex dental conditions.
a) Ethical advancements: Open data sharing promotes transparency and ethical data use. Researchers are more likely to adhere to ethical standards when their work is subject to scrutiny by the broader scientific community.
Collaborating with researchers and scientists
Collaboration between dentists and researchers or scientists specializing in AI and data analysis is essential for harnessing clinical data effectively [67,68]:
a) Interdisciplinary teams: Forming interdisciplinary teams that include dentists, data scientists, machine learning experts, and healthcare researchers ensures a well-rounded approach to AI modelling. Each team member brings unique skills and knowledge to the project.
b) Data expertise: Collaborating with data experts is crucial for data preprocessing, feature engineering, and algorithm development. Data scientists can assist in extracting valuable insights from clinical data.
c) Research partnerships: Establishing research partnerships with academic institutions or research organizations can provide access to cutting-edge AI methodologies and resources. These partnerships can lead to joint research projects and funding opportunities.
d) Continuous communication: Effective communication between dental practitioners and researchers is essential throughout the project. Dentists should convey clinical insights and domain-specific knowledge, while researchers can translate this information into AI models.
Overcoming barriers to data sharing
Despite the benefits of data sharing, there are challenges and barriers that need to be addressed [69,70]:
a) Data Privacy and Security: Ensuring patient data privacy and security is paramount. Dentists must implement robust data encryption, access controls, and de-identification techniques to protect sensitive information.
a) Regulatory Compliance: Adhering to healthcare data regulations like HIPAA is critical. Dentists and researchers must navigate regulatory requirements to ensure legal data sharing practices.
a) Data Ownership: Clarifying data ownership and consent issues is essential. Dentists should obtain informed consent from patients for data sharing and clearly define ownership agreements when collaborating with external partners.
a) Data Quality and Standardization: Maintaining data quality and standardization across different sources can be challenging. Dentists should establish data collection protocols and quality assurance measures.
a) Cultural Shif: Overcoming the cultural shift towards data sharing in healthcare is crucial. Dentists and healthcare institutions should promote a culture of data transparency and collaboration.
Open data sharing and collaboration between dentists and researchers are integral to harnessing clinical data for AI modelling in dentistry. Embracing these practices can lead to faster advancements, improved patient care, and the responsible and ethical development of AI-driven solutions in the dental field. Overcoming barriers and ensuring data privacy and security are essential for successful collaboration in this data-driven era of dentistry.
Overcoming bias and generalization issues
In the pursuit of harnessing clinical data for AI modelling in dentistry, it is essential to address bias and generalization issues. Bias in datasets and the failure of AI models to generalize effectively can lead to inaccurate or unfair outcomes [71]. This section discusses strategies for recognizing and mitigating bias in datasets and offers insights into strategies for generalizing AI models for improved patient care.
Recognizing and mitigating bias in datasets
Bias in datasets can arise from various sources, including disparities in patient demographics, unequal access to dental care, and systematic errors in data collection [72]. Recognizing and mitigating bias is crucial to ensure that AI models provide equitable and reliable results [73].
a) Data audit and evaluation: Dentists and data scientists should conduct a comprehensive audit of clinical data to identify potential sources of bias. This involves examining demographic imbalances, disparities in data collection methods, and any historical biases in the data. By understanding the biases present in the dataset, steps can be taken to mitigate their impact.
a) Diverse representation: Ensuring that the dataset represents a diverse patient population is essential to mitigate bias. Efforts should be made to collect data from a wide range of demographics, including age, gender, ethnicity, socioeconomic status, and geographic location. This diversity helps the AI model learn from a broader set of patient experiences and reduces the risk of biased outcomes.
a) Fair data collection practices: Dentists and data collectors should implement fair data collection practices to minimize bias during data entry. This includes standardized data collection procedures, clear guidelines for data recording, and ongoing training to reduce human error in data collection.
a) Algorithmic fairness: Data scientists should employ algorithms and techniques that promote fairness and equity. Fairness metrics can be used to assess model performance across different demographic groups. Adjustments to the model can be made to ensure that it does not disproportionately favor or harm any particular group.
a) Transparency and accountability: Dentists and researchers should prioritize transparency in AI model development. This includes documenting data preprocessing steps, algorithm choices, and any adjustments made to address bias. Accountability measures should be in place to review and address bias-related issues as they arise.
Strategies for generalizing AI models
Generalization is the ability of an AI model to apply what it has learned from one set of data to make accurate predictions on new, unseen data [74]. Generalization issues can arise when AI models overfit the training data or fail to adapt to variations in real-world patient cases. Strategies to enhance generalization in AI models include [75,76]:
a) Cross-validation: Cross-validation techniques, such as k-fold cross-validation, can help assess a model’s generalization performance. By splitting the data into multiple subsets for training and testing, cross-validation provides a more robust evaluation of a model’s ability to generalize to unseen data.
a) Regularization techniques: Regularization methods, like L1 and L2 regularization, can prevent overfitting by adding penalty terms to the model’s loss function. These penalties encourage the model to simplify its predictions, leading to better generalization.
a) Data augmentation: Data augmentation involves creating new training examples by applying random transformations or perturbations to the existing data. This technique can help the model learn from a wider range of data variations, improving its ability to generalize.
a) Ensemble learning: Ensemble learning involves combining multiple AI models to make predictions. By aggregating the outputs of several models, ensemble methods often achieve better generalization by reducing the impact of individual model biases or errors.
a) Transfer learning: Transfer learning allows AI models to leverage knowledge learned from one task or dataset to improve performance on a related task or dataset. Dentists can explore pre-trained models and adapt them for dental applications, reducing the need for large amounts of domain-specific data.
a) Real-world testing: AI models should undergo rigorous testing in real-world dental practice settings. Regular evaluations of the model’s performance on diverse patient cases ensure that it continues to generalize effectively and provide accurate insights.
a) Continuous learning: AI models should be designed for continuous learning and adaptation. As new clinical data becomes available, models can be updated and refined to maintain their generalization capabilities and adapt to evolving patient care needs.
Recognizing and mitigating bias in datasets and enhancing the generalization of AI models are essential steps in harnessing clinical data for AI modelling in dentistry. By addressing these issues, dentists and researchers can develop AI-driven solutions that provide equitable and accurate patient care while maintaining the highest standards of ethics and quality.
Best practices for data preservation and storage
Clinical data in dentistry, crucial for AI modelling and enhancing patient care, must be preserved, and stored securely to ensure its long-term accessibility and integrity. Implementing best practices for data preservation and storage is essential to safeguard this valuable resource.
Long-term data preservation
Long-term data preservation involves strategies to ensure that clinical data remains accessible and usable for extended periods, even as technology evolves. Dentists and researchers should consider the following best practices [77,78]:
a) Data standardization: Standardize data formats, coding schemes, and metadata to facilitate data interoperability and reduce the risk of data obsolescence. Using widely accepted data standards ensures that data can be interpreted and utilized by future AI systems and research.
a) Version control: Implement version control systems to track changes and updates to datasets. Maintaining a clear version history helps ensure data consistency and allows for the retrieval of previous dataset iterations if needed.
a) Data documentation: Create comprehensive data documentation that includes data dictionaries, data lineage, and descriptions of data collection processes. This documentation should be regularly updated to provide context for future users.
a) Data migration plans: Develop data migration strategies to transfer data from outdated storage systems or formats to newer ones. As technology advances, it’s crucial to have a plan for preserving and updating data to remain compatible with evolving AI models and tools.
a) Data preservation policies: Establish clear data preservation policies and assign responsibility for data stewardship. Dentists and research teams should define roles and responsibilities for data custodians and ensure ongoing commitment to data preservation efforts.
Data backup and redundancy measures
To protect clinical data from loss or corruption, implementing robust data backup and redundancy measures is essential [79,80]:
a) Regular backups: Regularly schedule automated backups of clinical data to prevent data loss due to hardware failures, system crashes, or accidental deletions. Backup frequency should be determined based on data volatility and importance.
a) Off-site storage: Store backup copies of clinical data off-site, preferably in geographically distant locations, to safeguard against disasters such as fires, floods, or physical theft. Cloud-based storage solutions with encryption can enhance data security and accessibility.
a) Redundant storage systems: Implement redundant storage systems, including redundant servers and storage devices, to ensure data availability in case of hardware failures. Employing a fault-tolerant architecture minimizes downtime and data loss.
a) Data validation: Regularly validate the integrity of backup copies through checksums or data validation techniques. This helps ensure that backed-up data remains consistent and free from corruption.
a) Disaster recovery plans: Develop comprehensive disaster recovery plans that outline procedures for data restoration in the event of a catastrophic data loss scenario. Test these plans periodically to verify their effectiveness.
a) Access control: Enforce strict access controls and permissions for clinical data, ensuring that only authorized personnel can access, modify, or delete data. Implement encryption to protect data during transmission and storage.
By adhering to best practices for data preservation and storage, dentists and researchers can safeguard clinical data’s longterm accessibility and reliability. These measures not only protect against data loss but also contribute to the responsible and ethical use of clinical data in AI modelling for enhanced patient care.
Future directions and emerging technologies
The evolution of AI in dentistry
The evolution of Artificial Intelligence (AI) in dentistry is poised to continue shaping the future of dental care in profound ways. As technology advances and AI algorithms become more sophisticated, several key trends and emerging technologies are likely to define the trajectory of AI in dentistry.
Enhanced diagnostic accuracy
AI algorithms have already demonstrated their potential in improving diagnostic accuracy in dentistry. In the future, we can expect even more advanced AI models capable of detecting subtle dental abnormalities and diseases with unprecedented precision [81]. This will enable earlier intervention, reducing the severity of oral health issues and improving patient outcomes.
Personalized treatment planning
The concept of personalized medicine is extending into dentistry. AI will play a pivotal role in tailoring treatment plans to individual patients’ needs, taking into account their medical history, genetics, oral health status, and preferences [82]. This approach will maximize treatment effectiveness and patient satisfaction.
Tele-dentistry and remote monitoring
Tele-dentistry, coupled with AI-powered remote monitoring, will become increasingly prevalent. Patients can receive realtime guidance on oral hygiene practices and track their treatment progress from the comfort of their homes. AI algorithms will analyse data from wearable devices and provide valuable insights to both patients and dental professionals [83].
Robotics in dental procedures
Robotic-assisted dental procedures will gain traction, with AI-driven robots assisting dentists in performing tasks with precision and accuracy. This can include tasks such as tooth extractions, implant placements, and even surgeries. Robotics will enhance procedural outcomes and reduce the margin for error [84].
AI-enhanced dental education
AI will revolutionize dental education by offering immersive, AI-powered simulations and training modules. Dental students and professionals can practice various procedures in virtual environments, honing their skills and gaining confidence before performing treatments on patients [85].
AI-driven predictive analytics in dental care
Early disease prediction
AI-driven predictive analytics will play a crucial role in identifying individuals at risk of dental diseases. By analysing extensive patient data, including genetic markers, lifestyle factors, and historical dental records, AI algorithms can pinpoint individuals who may be predisposed to specific oral health issues. Early intervention and preventive measures can then be implemented to mitigate these risks [86].
Treatment outcome prediction
Predictive analytics will also assist in estimating treatment outcomes with a high degree of accuracy. AI models can analyse patient data to predict the success rate of various treatment options, allowing dentists and patients to make informed decisions about their dental care. This will enhance treatment planning and optimize resource allocation [87].
Patient behaviour modelling
Understanding patient behaviour is crucial for promoting oral health. AI-driven predictive analytics can model patient behaviour patterns, helping dentists tailor their communication and education strategies to maximize patient compliance with recommended treatments and oral hygiene practices [88].
Resource allocation optimization
Dental practices can benefit from predictive analytics to optimize resource allocation. AI can predict patient appointment cancellations, assess equipment maintenance needs, and forecast patient influx to ensure efficient use of resources and minimal downtime [89-91].
The future of AI in dentistry promises continued growth and innovation. Enhanced diagnostic accuracy, personalized treatment planning, tele-dentistry, robotics, and AI-driven dental education are some of the exciting developments on the horizon. Additionally, the integration of predictive analytics into dental care will revolutionize disease prevention, treatment planning, patient behaviour modelling, and resource allocation. Dentists and dental professionals embracing these emerging technologies will be well-positioned to deliver higher-quality care and improved patient experiences in the years to come.
Conclusion
In conclusion, this paper has underscored the pivotal role of clinical data in harnessing the power of AI modelling for enhanced patient care in dentistry. We have highlighted the significance of quality clinical data, emphasizing that it serves as the foundation for AI algorithms, enabling them to provide accurate diagnoses, personalized treatment plans, and improved patient experiences. The paper discussed the importance of data collection methods, including electronic health records, imaging data, clinical notes, and patient surveys, while considering the challenges associated with each approach. Recapitulating key points, it is evident that AI has the potential to revolutionize dentistry by expediting diagnosis, enabling personalized treatment recommendations, and streamlining practice management. However, this potential can only be realized with the availability of high-quality, diverse, and well-curated clinical data. Dentists, as custodians of patient data, are encouraged to actively contribute to AI modelling by adhering to ethical standards, ensuring data privacy, and staying informed about data protection regulations. Looking ahead, the potential impact of AI in advancing dental care is vast. AI-driven dentistry can lead to early disease detection, improved treatment outcomes, and more efficient practice operations. It has the power to transform how dental care is delivered, ultimately benefiting both patients and practitioners. Dentists should embrace this transformative technology, collaborate with data scientists, and continue to explore innovative ways to leverage clinical data for the betterment of dental healthcare. By doing so, they can be at the forefront of a new era in dentistry, where AI enhances patient care and reshapes the future of the profession.
References
- Sadegh-Zadeh, Seyed-Ali, Mahboobe Bahrami, Amirreza Najafi, Meisam Asgari-Ahi, et al. Evaluation of COVID-19 Pandemic on Components of Social and Mental Health Using Machine Learning, Analysing United States Data in 2020. Frontiers in Psychiatry. 2022; 13.
- Alshadidi, Abdulkhaliq Ali F, Ahid Amer Alshahrani, Lujain Ibrahim N Aldosari, Saurabh Chaturvedi, et al. Investigation on the Application of Artificial Intelligence in Prosthodontics. Applied Sciences. 2023; 13(8): 5004.
- Abu Salim, Samah, Nordin Zakaria, Md Rafiqul Islam, Ganesh Kumar, et al. Analysis of Deep Learning Techniques for Dental Informatics: A Systematic Literature Review. In Healthcare. 2022; 10: 1892. MDPI.
- Ezhov, Matvey, Maxim Gusarev, Maria Golitsyna, Julian M Yates, et al. Clinically Applicable Artificial Intelligence System for Dental Diagnosis with CBCT. Scientific Reports. 2021; 11(1): 15006.
- Dayan, Ittai, Holger R Roth, Aoxiao Zhong, Ahmed Harouni, et al. Federated Learning for Predicting Clinical Outcomes in Patients with COVID-19. Nature Medicine. 2021; 27(10): 1735-43.
- Bhardwaj, Abhaya, Shristi Kishore, Dhananjay K Pandey. Artificial Intelligence in Biological Sciences. Life. 2022; 12(9): 1430.
- O’Leary, Colin P, Matthew A Cavender. Emerging Opportunities to Harness Real World Data: An Introduction to Data Sources, Concepts, and Applications. Diabetes, Obesity and Metabolism. 2022; 22: 3-12.
- Alshenqeeti, Hamza. Interviewing as a Data Collection Method: A Critical Review. English Linguistics Research. 2014; 3(1): 39-45.
- Cicero, Theodore J, Matthew S Ellis, Hilary L Surratt, Steven P Kurtz. The Changing Face of Heroin Use in the United States: A Retrospective Analysis of the Past 50 Years. JAMA Psychiatry. 2014; 71(7): 821-26.
- Corey, Kristin M, Sehj Kashyap, Elizabeth Lorenzi, Sandhya A Lagoo-Deenadayalan, et al. Development and Validation of Machine Learning Models to Identify High-Risk Surgical Patients Using Automatically Curated Electronic Health Record Data (Pythia): A Retrospective, Single-Site Study. PLoS Medicine. 2018; 15(11): e1002701.
- Wells, Brian J, Kevin M Chagin, Amy S Nowacki, Michael W Kattan. Strategies for Handling Missing Data in Electronic Health Record Derived Data. Egems. 2013; 1(3).
- Strober, Michael, Roberta Freeman, Wendy Morrell. The Long‐term Course of Severe Anorexia Nervosa in Adolescents: Survival Analysis of Recovery, Relapse, and Outcome Predictors over 10-15 Years in a Prospective Study. International Journal of Eating Disorders.1997; 22(4): 339-60.
- Fossey, Ellie, Carol Harvey, Fiona McDermott, Larry Davidson. Understanding and Evaluating Qualitative Research. Australian & New Zealand Journal of Psychiatry. 2002; 36(6): 717-32.
- Asan, Onur, Avishek Choudhury. Research Trends in Artificial Intelligence Applications in Human Factors Health Care: Mapping Review. JMIR Human Factors. 2021; 8(2): e28236.
- Walker, Alan, and Mark Teaford. Inferences from Quantitative Analysis of Dental Microwear. Folia Primatologica. 1989; 53(1-4): 177-89.
- Ahmed, Rafay, Matthew J Oborski, Misun Hwang, Frank S Lieberman, et al. Malignant Gliomas: Current Perspectives in Diagnosis, Treatment, and Early Response Assessment Using Advanced Quantitative Imaging Methods. Cancer Management and Research. 2014; 149-70.
- Salehi, Hassan S, Mina Mahdian, Mohammad M Murshid, Stefan Judex, et al. Deep Learning-Based Quantitative Analysis of Dental Caries Using Optical Coherence Tomography: An Ex Vivo Study. In Lasers in Dentistry. 2019; 10857: 39-46. SPIE.
- Miller, D Douglas, and Eric W Brown. Artificial Intelligence in Medical Practice: The Question to the Answer? The American Journal of Medicine. 2018; 131(2): 129-33.
- Schwendicke F, et al, W Samek, J Krois. Artificial Intelligence in Dentistry: Chances and Challenges. Journal of Dental Research. 2020; 99(7): 769-74.
- Esmaeilzadeh, Pouyan. Use of AI-Based Tools for Healthcare Purposes: A Survey Study from Consumers’ Perspectives. BMC Medical Informatics and Decision Making. 2020; 20(1): 1-19.
- Hansen E. HIPAA (Health Insurance Portability and Accountability Act) Rules: Federal and State Enforcement. Medical Interface. 1997; 10(8): 96-98.
- Regulation, General Data Protection. General Data Protection Regulation (GDPR). Intersoft Consulting, Accessed in October. 2018; 24(1).
- Rahul Kumar, Rohitash Kumar Banyal. Data Life Cycle Management in Big Data Analytics. Procedia Computer Science. 2020; 173: 364-71.
- Sadegh-Zadeh, Seyed-Ali. Computational Methods toward Early Detection of Neuronal Deterioration. University of Hull. 2019.
- Johnson, Kevin B, Wei‐Qi Wei, Dilhan Weeraratne, Mark E Frisse, et al. Precision Medicine, AI, and the Future of Personalized Health Care. Clinical and Translational Science. 2021; 14(1): 86-93.
- Bird Alix, Lauren Oakden-Rayner, Christopher McMaster, Luke A Smith, Minyan Zeng, et al. Artificial Intelligence and the Future of Radiographic Scoring in Rheumatoid Arthritis: A Viewpoint. Arthritis Research & Therapy. 2022; 24(1): 1-10.
- Dhopte Ashwini, Hiroj Bagde. Smart Smile: Revolutionizing Dentistry with Artificial Intelligence. Cureus. 2023; 15(6).
- Thurzo Andrej, Martin Strunga, Renáta Urban, Jana Surovková, Kelvin I Afrashtehfar. Impact of Artificial Intelligence on Dental Education: A Review and Guide for Curriculum Update. Education Sciences. 2023; 13(2): 150.
- Rokhshad, Rata, Maxime Ducret, Akhilanand Chaurasia, Teodora Karteva, Miroslav Radenkovic, Jelena Roganovic, Manal Hamdan, Hossein Mohammad-Rahimi, Joachim Krois, and Pierre Lahoud. Ethical Considerations on Artificial Intelligence in Dentistry: A Framework and Checklist. Journal of Dentistry. 2023; 104593.
- Sadegh-Zadeh, Seyed-Ali, Chandrasekhar Kambhampati. 2018. Computational Investigation of Amyloid Peptide Channels in Alzheimer’s Disease. J. 2018; 2(1): 1-14.
- Sadegh-Zadeh, Seyed-Ali, Chandrasekhar Kambhampati, and Darryl N Davis. Ionic Imbalances and Coupling in Synchronization of Responses in Neurons. J. 2019; 2(1): 17-40.
- Sadegh-Zadeh, Seyed-Ali, Elham Fakhri, Mahboobe Bahrami, Elnaz Bagheri, et al. An Approach toward Artificial Intelligence Alzheimer’s Disease Diagnosis Using Brain Signals. Diagnostics. 2023; 13(3): 477.
- Commissioner, Ontario. Office of the Information and Privacy, Ann Cavoukian, and Daniel Castro. Big Data and Innovation, Setting the Record Straight: De-Identification Does Work. Information and Privacy Commissioner, Ontario. 2014.
- Sadegh-Zadeh, Seyed-Ali, Ali Rahmani Qeranqayeh, Elhadj Benkhalifa, David Dyke, et al. Dental Caries Risk Assessment in Children 5 Years Old and under via Machine Learning. Dentistry Journal. 2022; 10(9): 164.
- Vovk, Olga, Gunnar Piho, Peeter Ross. Methods and Tools for Healthcare Data Anonymization: A Literature Review. International Journal of General Systems. 2023; 52(3): 326-42.
- Carrillo‐Perez, Francisco, Oscar E Pecho, Juan Carlos Morales, Rade D Paravina, et al Applications of Artificial Intelligence in Dentistry: A Comprehensive Review. Journal of Esthetic and Restorative Dentistry. 2022; 34(1): 259-80.
- Hung Man, Jungweon Park, Eric S Hon, Jerry Bounsanga, Sara Moazzami, et al. Artificial Intelligence in Dentistry: Harnessing Big Data to Predict Oral Cancer Survival. World Journal of Clinical Oncology. 2020; 11(11): 918.
- Rieke Nicola, Jonny Hancox, Wenqi Li, Fausto Milletari, Holger R Roth, et al. The Future of Digital Health with Federated Learning. NPJ Digital Medicine. 2020; 3(1): 119.
- Tayefi Maryam, Phuong Ngo, Taridzo Chomutare, Hercules Dalianis, Elisa Salvi, et al. Challenges and Opportunities beyond Structured Data in Analysis of Electronic Health Records. Wiley Interdisciplinary Reviews: Computational Statistics. 2021; 13(6): e1549.
- Sadegh-Zadeh, Seyed-Ali, Hanie Sakha, Sobhan Movahedi, Aniseh Fasihi Harandi, et al. Advancing Prognostic Precision in Pulmonary Embolism: A Clinical and Laboratory-Based Artificial Intelligence Approach for Enhanced Early Mortality Risk Stratification. Computers in Biology and Medicine. 2023; 107696.
- Bois, A H Du, B Kardachi, P M Bartold. Is There a Role for the Use of Volumetric Cone Beam Computed Tomography in Periodontics? Australian Dental Journal. 2012; 57: 103-8.
- Häyrinen, Kristiina, Kaija Saranto, Pirkko Nykänen. Definition, Structure, Content, Use and Impacts of Electronic Health Records: A Review of the Research Literature. International Journal of Medical Informatics. 2008; 77(5): 291-304.
- Mc Coll, Elaine, Ann Jacoby, Lois Thomas, Jennifer Soutter, et al. Design and Use of Questionnaires: A Review of Best Practice Applicable to Surveys of Health Service Staff and Patients. 2001.
- Kang, In-Ae, Soualihou Ngnamsie Njimbouom, Kyung-Oh Lee, Jeong-Dong Kim. DCP: Prediction of Dental Caries Using Machine Learning in Personalized Medicine. Applied Sciences. 2022; 12(6): 3043.
- Alasadi, Suad A, Wesam S Bhaya. Review of Data Preprocessing Techniques in Data Mining. Journal of Engineering and Applied Sciences. 2017; 12(16): 4102-7.
- Dziura, James D, Lori A Post, Qing Zhao, et al. Strategies for Dealing with Missing Data in Clinical Trials: From Design to Analysis. The Yale Journal of Biology and Medicine. 2013; 86 (3): 343.
- Bornstein, Marc H, Justin Jager, and Diane L Putnick. 2013. Sampling in Developmental Science: Situations, Shortcomings, Solutions, and Standards. Developmental Review 33 (4): 357-70.
- Suresh, Harini, and John Guttag. 2021. A Framework for Understanding Sources of Harm throughout the Machine Learning Life Cycle. In Equity and Access in Algorithms, Mechanisms, and Optimization, 1-9.
- Zhang Ling, Xiaosong Wang, Dong Yang, Thomas Sanford, Stephanie Harmon, et al. Generalizing Deep Learning for Medical Image Segmentation to Unseen Domains via Deep Stacked Transformation. IEEE Transactions on Medical Imaging. 2020; 39(7): 2531-40.
- Ng Dianwen, Xiang Lan, Melissa Min-Szu Yao, Wing P Chan, Mengling Feng. Federated Learning: A Collaborative Effort to Achieve Better Medical Imaging Models for Individual Sites That Have Small Labelled Datasets. Quantitative Imaging in Medicine and Surgery. 2021; 11(2): 852.
- Martinez-Garcia Mireya, Enrique Hernández-Lemus. Data Integration Challenges for Machine Learning in Precision Medicine. Frontiers in Medicine. 2022; 8: 784455.
- Vignaux Laurence, Frédéric Vargas, Jean Roeseler, Didier Tassaux, Arnaud W Thille, et al. Patient-Ventilator Asynchrony during Non-Invasive Ventilation for Acute Respiratory Failure: A Multicenter Study. Intensive Care Medicine. 2009; 35: 840-46.
- He Jianxing, Sally L Baxter, Jie Xu, Jiming Xu, Xingtao Zhou, et al. The Practical Implementation of Artificial Intelligence Technologies in Medicine. Nature Medicine. 2019; 25(1): 30-36.
- Lehne Moritz, Julian Sass, Andrea Essenwanger, Josef Schepers, Sylvia Thun. Why Digital Medicine Depends on Interoperability. NPJ Digital Medicine. 2019; 2(1): 79.
- Walji, Muhammad F, Elsbeth Kalenderian, Duong Tran, Krishna K Kookal, Vickie Nguyen, et al. Detection and Characterization of Usability Problems in Structured Data Entry Interfaces in Dentistry. International Journal of Medical Informatics. 2013; 82(2): 128-38.
- Association, American Dental. CDT 2023: Current Dental Terminology. American Dental Association. 2022.
- Pietro Carlo De, Igor Francetic. E-Health in Switzerland: The Laborious Adoption of the Federal Law on Electronic Health Records (EHR) and Health Information Exchange (HIE) Networks. Health Policy. 2018; 122 (2): 69-74.
- Strasberg, Howard R, Bryn Rhodes, Guilherme Del Fiol, Robert A Jenders, et al. Contemporary Clinical Decision Support Standards Using Health Level Seven International Fast Healthcare Interoperability Resources. Journal of the American Medical Informatics Association. 2021; 28(8): 1796-1806.
- Lim Jinho, Rashad Zein. The Digital Imaging and Communications in Medicine (DICOM): Description, Structure and Applications. Rapid Prototyping: Theory and Practice. 2006; 63-86.
- Garg Shivank, Noelle L Williams, Andrew Ip, Adam P Dicker. Clinical Integration of Digital Solutions in Health Care: An Overview of the Current Landscape of Digital Technologies in Cancer Care. JCO Clinical Cancer Informatics. 2018; 2: 1-9.
- Gupta Nitu, Katpagavalli Anantharaj, Karthikeyan Subramani. Containerized Architecture for Edge Computing in Smart Home: A Consistent Architecture for Model Deployment. In 2020 International Conference on Computer Communication and Informatics (ICCCI). 2020; 1-8. IEEE.
- Ayaz Muhammad, Muhammad F Pasha, Mohammed Y Alzahrani, Rahmat Budiarto, Deris Stiawan. The Fast Health Interoperability Resources (FHIR) Standard: Systematic Literature Review of Implementations, Applications, Challenges and Opportunities. JMIR Medical Informatics. 2021; 9(7): e21929.
- Dagher Gaby G, Jordan Mohler, Matea Milojkovic, Praneeth Babu Marella. Ancile: Privacy-Preserving Framework for Access Control and Interoperability of Electronic Health Records Using Blockchain Technology. Sustainable Cities and Society. 2018; 39: 283-97.
- Murray-Rust, Peter. Open Data in Science. Nature Precedings. 2008; 1.
- Byrd James Brian, Anna C Greene, Deepashree Venkatesh Prasad, Xiaoqian Jiang, Casey S Greene. Responsible, Practical Genomic Data Sharing That Accelerates Research. Nature Reviews Genetics. 2020; 21(10): 615-29.
- Hardwicke, Tom E, Maya B Mathur, Kyle MacDonald, Gustav Nilsonne, et al. Data Availability, Reusability, and Analytic Reproducibility: Evaluating the Impact of a Mandatory Open Data Policy at the Journal Cognition. Royal Society Open Science. 2018; 5(8): 180448.
- Park Sun Young, Pei-Yi Kuo, Andrea Barbarin, Elizabeth Kaziunas, Astrid Chow, et al. Identifying Challenges and Opportunities in Human-AI Collaboration in Healthcare. In Conference Companion Publication of the 2019 on Computer Supported Cooperative Work and Social Computing. 2019; 506-10.
- Wang Dakuo, Justin D Weisz, Michael Muller, Parikshit Ram, Werner Geyer, et al. Human-Ai Collaboration in Data Science: Exploring Data Scientists’ Perceptions of Automated Ai. Proceedings of the ACM on Human-Computer Interaction 3 (CSCW). 2019; 1-24.
- Óh Éigeartaigh, Seán S, Jess Whittlestone, Yang Liu, Yi Zeng, et al. Overcoming Barriers to Cross-Cultural Cooperation in AI Ethics and Governance. Philosophy & Technology. 2020; 33: 571-93.
- DuMont Schütte, August, Jürgen Hetzel, Sergios Gatidis, Tobias Hepp, et al. Overcoming Barriers to Data Sharing with Medical Image Generation: A Comprehensive Evaluation. NPJ Digital Medicine. 2021; 4(1): 141.
- Roselli Drew, Jeanna Matthews, Nisha Talagala. Managing Bias in AI. In Companion Proceedings of the 2019 World Wide Web Conference. 2019; 539-44.
- Norori Natalia, Qiyang Hu, Florence Marcelle Aellen, Francesca Dalia Faraci, Athina Tzovara. Addressing Bias in Big Data and AI for Health Care: A Call for Open Science. Patterns. 2021; 2(10).
- Gianfrancesco Milena A, Suzanne Tamang, Jinoos Yazdany, Gabriela Schmajuk. Potential Biases in Machine Learning Algorithms Using Electronic Health Record Data. JAMA Internal Medicine. 2018; 178(11): 1544-47.
- Ridhawi, Ismaeel Al, Safa Otoum, Moayad Aloqaily, Azzedine Boukerche. Generalizing AI: Challenges and Opportunities for Plug and Play AI Solutions. IEEE Network. 2020; 35(1): 372-79.
- Zunino, Andrea, Sarah Adel Bargal, Riccardo Volpi, Mehrnoosh Sameki, Jianming Zhang, Stan Sclaroff, Vittorio Murino, and Kate Saenko. 2021. Explainable Deep Classification Models for Domain Generalization. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, 3233-42.
- Srinivas, Sampath. A Generalization of the Noisy-or Model. In Uncertainty in Artificial Intelligence. 1993; 208-15.
- Lorie, Raymond A. Long Term Preservation of Digital Information. In Proceedings of the 1st ACM/IEEE-CS Joint Conference on Digital Libraries. 2001; 346-52.
- Bhat, Wasim Ahmad. Long-Term Preservation of Big Data: Prospects of Current Storage Technologies in Digital Libraries. Library Hi Tech. 2018; 36(3): 539-55.
- Gill Phillipa, Navendu Jain, Nachiappan Nagappan. Understanding Network Failures in Data Centers: Measurement, Analysis, and Implications. In Proceedings of the ACM SIGCOMM 2011 Conference. 2011; 350-61.
- Meister Dirk, André Brinkmann. Multi-Level Comparison of Data Deduplication in a Backup Scenario. In Proceedings of SYSTOR 2009: The Israeli Experimental Systems Conference. 2009; 1-12.
- Nguyen, Thomas T, Naomie Larrivée, Alicia Lee, Olexa Bilaniuk, et al. Use of Artificial Intelligence in Dentistry: Current Clinical Trends and Research Advances. J Can Dent Assoc. 2021; 87(l7): 1488-2159.
- Shujaat, Sohaib, Marryam Riaz, and Reinhilde Jacobs. Synergy between Artificial Intelligence and Precision Medicine for Computer-Assisted Oral and Maxillofacial Surgical Planning. Clinical Oral Investigations. 2023; 27(3): 897-906.
- Ghai Suhani. Teledentistry during COVID-19 Pandemic. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2020; 14(5): 933-35.
- Wu, Yiqun, Feng Wang, Shengchi Fan, and James Kwok-Fai Chow. 2019. Robotics in Dental Implantology. Oral and Maxillofacial Surgery Clinics. 2019; 31(3): 513-18.
- Gowthaman Aadithya, Linda Kirova, L BingYu, Patrick Molen, Ines Said, et al. Immersive Learning with AI-Enhanced Virtual Standardized Patient (VSP) to Improve Dental Student’s Communication Proficiencies. In The 14th International Conference on Advances in Computer-Human Interactions. 2021.
- Hung, Kuo Feng, Andy Wai Kan Yeung, Michael M Bornstein, Falk Schwendicke. Personalized Dental Medicine, Artificial Intelligence, and Their Relevance for Dentomaxillofacial Imaging. Dentomaxillofacial Radiology. 2023; 52(1): 20220335.
- Chen, Yo-wei, Kyle Stanley, Wael Att. Artificial Intelligence in Dentistry: Current Applications and Future Perspectives. Quintessence Int. 2020; 51(3): 248-57.
- Xu Boyi, Ling Li, Daiping Hu, Bin Wu, Congcong Ye, et al. Healthcare Data Analysis System for Regional Medical Union in Smart City. Journal of Management Analytics. 2018; 5(4): 334-49.
- Grover Varun, Roger H L Chiang, Ting-Peng Liang, Dongsong Zhang. Creating Strategic Business Value from Big Data Analytics: A Research Framework. Journal of Management Information Systems. 2018; 35(2): 388-423.
- Mathauer Inke, Ingo Imhoff. Health Worker Motivation in Africa: The Role of Non-Financial Incentives and Human Resource Management Tools. Human Resources for Health. 2006; 4(1): 1-17.
- Sivarajah Uthayasankar, Muhammad Mustafa Kamal, Zahir Irani, Vishanth Weerakkody. Critical Analysis of Big Data Challenges and Analytical Methods. Journal of Business Research. 2017; 70: 263-86.