
Open Journal of Clinical and
Medical Images
Clinical Image - Open Access, Volume 4
To bleed or to clot? The challenging coagulopathy of liver disease
Joel Thio1,2*; Jeevithan Sabanathan1,3
1Department of Gastroenterology and Hepatology, Logan Hospital, Queensland, Australia.
2Faculty of Medicine, University of Queensland, Brisbane, Australia.
3Faculty of Medicine, Griffith University, Brisbane, Australia.
*Corresponding Author: Joel Thio
Department of Gastroenterology and Hepatology, Logan Hospital, Queensland, Australia.
Email: joel_thio@hotmail.com
Received : Aug 08, 2024
Accepted : Sep 10, 2024
Published : Sep 17, 2024
Archived : www.jclinmedimages.org
Copyright : © Thio J (2023).
Abstract
Patients with liver cirrhosis present with the challenge of managing bleeding and prothrombotic complications of the disease. Portal vein thrombosis is a common complication of liver cirrhosis, with patients presenting with or without symptoms. The mainstay of treatment is anticoagulation, however, with the increased risk of bleeding. We present a case of a 43-year-old female who presented with haematemesis from a variceal bleed that was managed with endoscopic variceal banding, who subsequently developed acute portal venous and superior mesenteric vein thrombosis after worsening abdominal pain post-procedurally with a right-sided cerebellar haemorrhage which contraindicated anticoagulation. The complications of bleeding and thrombosis in liver cirrhosis limit management options in such patients, and hence illustrates the challenging coagulopathy of liver disease.
Citation: Thio J, Sabanathan J. To bleed or to clot? The challenging coagulopathy of liver disease. Open J Clin Med Images. 2024; 4(2): 1193.
Introduction
Cirrhosis of the liver is complicated by its ability to cause both prothrombotic and antithrombotic changes. Portal Vein Thrombosis (PVT) is a common prothrombotic complication of liver cirrhosis which may be complete or partial. Additionally, thrombosis can also involve the mesenteric and splenic veins. Many patients present asymptomatically, but a subgroup of patients present with complications such as mesenteric ischemia [1]. Alternatively, antithrombotic complications include spontaneous haematomas, variceal bleeding, and post-procedural bleeding [2]. We present a case of concurrent portal vein thrombosis and spontaneous intracerebral haemorrhage in a cirrhotic patient, further illustrating this paradigm and challenges of management.
Case report
A 43-year-old female with Child-Pugh B Hepatitis C-related cirrhosis presented to our centre with haematemesis. A Computer Tomographic (CT) scan of her abdomen on admission revealed evidence of liver cirrhosis with extensive portosystemic varices and a patent portal vein. She had a recorded haemoglobin of 112 g/L, platelet count of 155x109/L, and INR of 1.4. An urgent gastroscopy was undertaken and revealed grade III varices, with recent stigmata of bleeding, which were banded. Following gastroscopy, a CT scan of her head was performed for drowsiness. This scan was reported as being normal.
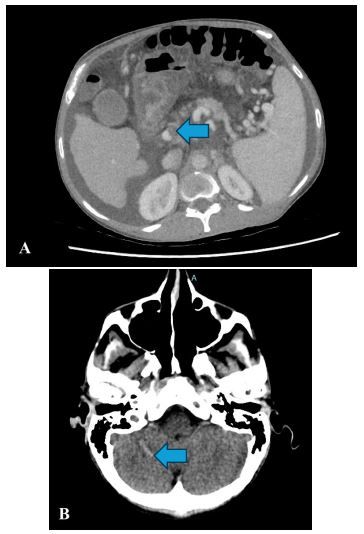
Over the next three days, the patient became progressively more drowsy despite appropriate management for hepatic encephalopathy, and also developed abdominal pain. Repeat CT head and abdomen were performed and unfortunately demonstrated new non-occlusive PVT (Figure 1A) and occlusive Superior Mesenteric Vein (SMV) thrombus, with marked mural thickening of the distal small bowel, and concurrent right-sided cerebellar haemorrhage (Figure 1B).
Management options in this instance were limited by concurrent bleeding and thrombosis. Her condition unfortunately continued to deteriorate and a decision was made to palliate following extensive discussion within a multidisciplinary team and the patient’s family.
Discussion
This case highlights the difficulties of managing the complications of bleeding and hypercoagulability in patients with liver cirrhosis. In our patient, her intracerebral haemorrhage occurred spontaneously with no previous trauma, aneurysms, genetic risk factors, or anticoagulation.
Development of PVT and SMV thrombus are known complications of liver disease, but there is growing suggestion that endoscopic variceal therapy could increase the risk of developing portal venous system thrombosis [3,4]. Given the acuity of thrombosis, her recent banding of varices could have contributed to the development of this, presumably from increasing portal pressures, worsening venous stasis and hence thrombosis.
The complications of bleeding and thrombosis in liver cirrhosis limit management options in such patients, and hence illustrates the challenging coagulopathy of liver disease.
References
- Garzelli L, Ben Abdallah I, Nuzzo A, Zappa M, Corcos O, et al. Insights into acute mesenteric ischaemia: An up-to-date, evidence-based review from a mesenteric stroke centre unit. The British Journal of Radiology. 2023; 96(1151): 20230232. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10607400/
- Rautou PE, Caldwell SH, Villa E. Bleeding and Thrombotic Complications in Patients with Cirrhosis: A State-of-the-Art Appraisal. Clin Gastroenterol Hepatol. 2023; 21(8): 2110-23.
- Wang L, Guo X, Xu X, Philips CA, Primignani M, et al. Association of portal venous system thrombosis with endoscopic variceal treatment: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2021; 32(2): 125-31.
- Wang L, Guo X, Shao X, Xu X, Zheng K, et al. Association of endoscopic variceal treatment with portal venous system thrombosis in liver cirrhosis: A case-control study. Therap Adv Gastroenterol. 2022; 15: 17562848221087536.