
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 4
Doctor, I can’t move my arms: Bilateral osteonecrosis of the humeral head
Iribar Dieguez Ion Koldobika1*; Sánchez Zugasti Belén2; González Santo Tomás Ruth2
1Emergency Service, Bidasoa Regional Hospital, Hondarribia, Guipúzcoa, Spain.
2Lesaka Health Center, Navarra, Spain
*Corresponding Author: Ion Koldobika ID
Emergency Service, Bidasoa Regional Hospital, Hondarribia, Guipúzcoa, Spain.
Email: ionkiribar@yahoo.es
Received : Sep 03, 2024
Accepted : Sep 27, 2024
Published : Oct 04, 2024
Archived : www.jclinmedimages.org
Copyright : © Iribar Dieguez IK (2023).
Abstract
Osteonecrosis of the humeral head is not as common as that of the femoral head, and its usual clinical manifestations: pain and functional limitation, are common to other diseases that are part of the so-called “painful shoulder”. Therefore, in the overall assessment of the shoulder, we must not forget the assessment of this pathology.
Citation: Iribar Dieguez IK, Sánchez Zugasti B, González Santo Tomás R. Doctor, I can’t move my arms: Bilateral osteonecrosis of the humeral head. Open J Clin Med Images. 2024; 4(2): 1194.
Introduction
Early detection and diagnosis of osteonecrosis of the humeral head are crucial to ensure early and effective treatment.
Case Report
Doctor, I can’t lift my arms!
An 86-year-old patient, unknown to our group, who, in the context of a consultation for another reason, reports difficulty and pain in moving her left arm, which is very swollen and without previous trauma. Her left arm is her only useful arm because she has not been able to move her right arm for more than 10 years.
On examination, the right shoulder appeared to be in an epaulette shape, with absolute inability for active mobilization and painless on passive mobilization, with normal distal sensitivity and pulse; the left shoulder, on the other hand, showed significant swelling, of adenomatous consistency, with very painful limitation for active mobility and also pain when attempting passive mobilization, with preserved distal neurovascular examination. Clinical ultrasound showed abundant hypoechoic material, causing distension of the capsule and deformation of its limits.
Based on these findings, arthrocentesis of 140cc of serosanguineous synovial fluid was performed.
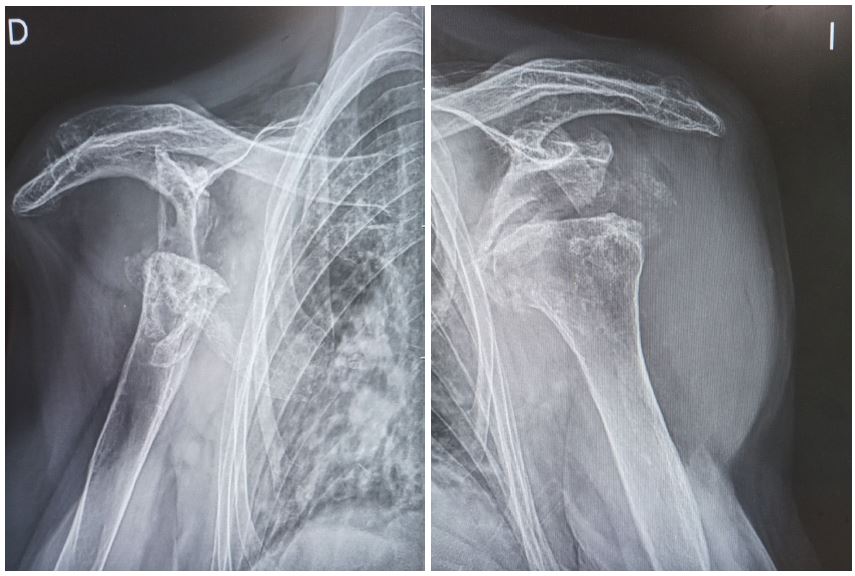
After this, a simple X-ray of both shoulders is requested (Figure 1).
Discussion
How is it possible that this patient was not detected earlier? Has she not consulted before and repeatedly for pain and functional limitation of the right arm first and then the left?
Etiologies and pathophysiology
Osteonecrosis (ON) is a pathological process that causes the death of cellular elements of bone. There is no consensus on its pathogenesis, although the common end result is reduced blood supply to the bone, increased intraosseous pressure, and bone death [1-6].
The etiology of osteonecrosis is multifactorial [4].
There may be no identified cause (primary or idiopathic ON). In 70% of ON of the humeral head (ONHH) no specific cause is found [7].
It may be related to some risk factor (secondary ON). Post-traumatic etiology is the most frequent. In the specific case of ONHH, when the cause is recognized, the use of corticosteroids is the most common [4].
There are numerous causes described in the literature [1]:
Traumatic (usually unilateral): Proximal humerus fractures-dislocations treated with osteosynthesis.
Non-traumatic (usually bilateral):
Endocrine/metabolic disorders
Gaucher disease: An enzyme deficiency causes the accumulation of glucocerebroside in macrophages, and an infiltration of the bone marrow with vascular compromise. It is the most frequent cause when patients have previously been splenectomised.
Hematologic disorders
Sickle cell anaemia [8]: autosomal recessive disorder common especially in blacks.
Extrinsic disorders
Dysbaric disorders (Caisson disease): Vascular involvement occurs due to decompression, and is related to depth, time under pressure and ascent speed.
Alcohol consumption: The connection between alcohol consumption and ONHH is known, but the mechanism by which it occurs is unknown.
Iatrogenic factors
Long-term use of corticosteroids [9]: They are a very common cause of non-traumatic ONHH, but the mechanism is unknown.
Miscellany
Rheumatic disorders, such as Systemic Lupus Erythematosus [1].
Organ transplantation [1].
Oncological disorders [10,11]: associated with Chronic Myeloid Leukaemia.
Hypercoagulant states [10].
- Hepatitis B and C, and the therapeutic use of pegylated interferon in them, are related to the presence of hypercoagulable states.
- Autoimmune disorders that may lead to transient vasculitis.
- Disorders related to the CoVID-19 vaccine [12].
Clinic
The humeral head is the second most common site (7%) of non-traumatic ON after the femoral head [1,4,6], and it is rare for it to occur in isolation in this location [2,4,6]. Frequently and for different reasons, most cases of ONHH progress to late arthritic stages requiring surgical intervention [13].
Non-traumatic ONHH presents with deep, insidious, pulsating pain radiating to the elbow, related to movement and limitation of movement [6,7]. Nocturnal pain is uncommon, and symptoms are limiting in 80% of patients [1]. In short, these are very non-specific symptoms shared by shoulder pain of any origin [4], but which, over time, generate significant morbidity [5], making it a disease that requires a high degree of suspicion [1].
arExploration [1]
Physical examination may reveal tenderness on palpation. Movement is usually preserved until the later stages, with active mobility being restricted and passive mobility being preserved [7]. Discomfort is greater with the arm abducted or elevated 90 degrees, which corresponds to the maximum glenohumeral load.
Complementary tests [1,7]
The diagnosis is clinical and radiographic.
Following clinical suspicion, plain radiography is the next step in diagnosis. At a very early stage of the disease, the disease may be undetectable with this technique. Early on, the term “crescent sign” describes an area of subchondral lucency in the humeral head indicating a fracture due to bone necrosis and subsequent attempts at repair. Later stages of ONHH are best assessed, showing progressive flattening of the humeral head, collapse, and degenerative changes.
Magnetic Resonance Imaging (MRI) is the diagnostic modality of choice. The diagnosis of ON on MRI is based on the presence of abnormal band-like signals and hypointense areas on T1. It has a sensitivity and specificity of 99% for detecting early ON of the shoulder [4]. It allows the assessment of the presence of joint effusion.
Computed axial Tomography (CT) may be useful in advanced stages of the disease.
Analyses such as complete blood count, erythrocyte sedimentation rate, C-reactive protein, or serologies may be useful to rule out or assess possible etiologies when the history is not clear.
Classification [1,4,7]
Staging of the disease using radiographs and MRI is predictive of disease progression and can help the orthopaedic surgeon guide treatment [2].
ONHH is usually classified using the Cruess scale and is divided into 5 stages:
| Stage 1 | Normal X-rays, positive MRI |
| Stage 2 | Sclerosis with preserved humeral head architecture |
| Stage 3 | Subchondral crescentic fracture (best seen in external rotation), ± collapse |
| Stage 4 | More advanced collapse with degenerative osteoarthritis and decreased joint space; normal glenoid |
| Stage 5 | Degenerative osteoarthritis of the humeral head and glenoid |
Treatment [1,2,5-7,13]
There is no therapeutic standard for the early stages of the disease (stage 1 and 2). In these phases, conservative treatments can be chosen, however, patients must be informed about the risk of progression of the disease to arthritic stages despite this:
- Nonsteroidal anti-inflammatory drugs and physical therapy can relieve painful range of motion.
- Bisphosphonates can prevent disease progression, bone collapse and the need for surgery.
As ONHH progresses and the collapse deteriorates the humeral head, the response to conservative treatment is worse and interventional measures are required:
- In intermediate phases, spinal cord decompression techniques have been described: a percutaneous technique using a deltopectoral approach and an arthroscopic technique, with or without chondral grafts.
- After collapse, the indication is usually arthroplasty: hemiarthroplasty or total arthroplasty depending on the glenoid status and the surgeon’s opinion.
Prognosis
The prognosis depends on the stage of the disease at the time of diagnosis.
Conclusion
The fact that rotator cuff disorder is the most common diagnosis for a painful shoulder (85%), that the humeral heads are involved, not subjected to pressure, and therefore with a more latent pain and limitation than in the case of the femoral heads, the age of the patient (without work requirements), rural environment (where the limitations associated with age are normalized), may have jointly contributed to the diagnosis of ONHH in our patient having been masked for so long and to her having been progressively adapting her imitations, compensating those of the right arm with the left arm until this has reached a point of degeneration and limitation such that she has been completely incapacitated.
Thus, the purpose of this article is two fold:
- To provide an updated review of the available evidence on risk factors, diagnosis and treatment of ONHH.
- Remind physicians to be alert to the possible diagnosis of ONHH in patients with chronic shoulder pain, especially if etiologic risk factors coexist, but even in the absence of predisposing conditions, through a comprehensive review of the medical history and additional examinations, in order to provide appropriate treatment.
Declarations
The work does not present any conflicts of interest.
The work has not received any funding.
References
- Hernigou P, Hernigou J, Scarlat M. Shoulder Osteonecrosis: Pathogenesis, Causes, Clinical Evaluation, Imaging, and Classification. Orthop Surg. 2020; 12 (5): 1340-1349. https://doi.org/10.1111/os.12788
- Castillo Mercado JS, Rojas Lievano J, Zaldivar B, Barajas C, Fierro G, et al. Atraumatic osteonecrosis of the humeral head: Pathophysiology and current concepts of evaluation and treatment. JSES Rev Rep Tech. 2022; 2(3): 277-284. https://doi.org/10.1016/j.xrrt.2022.02.005
- Arbab D, König DP. Atraumatic Femoral Head Necrosis in Adults. Dtsch Arztebl Int. 2016; 113(3): 31-38. https://doi.org/10.3238/arztebl.2016.0031
- Morán Hevia M, Redondo Buil P, López Díaz MDV, Montes García A, Vicente Quílez M. Avascular necrosis of bone: A disease with a name and a surname: A disease with a name and a surname. 2018. https://piper.espacio-seram.com/index.php/seram/article/view/123
- Lee WQ, Lie HM, Lie DTT. Diagnosis and treatment of avascular necrosis of the humeral head: Current concepts. J ISAKOS. 2023; 8(2): 108-113. https://doi.org/10.1016/j.jisako.2022.11.002
- Kuo FY, Chen KL, Yen CC. Idiopathic humeral head osteonecrosis mimicking rotator cuff disorders: Two challenging diagnostic case reports. Medicine (Baltimore). 2020; 99(3): e18766. https://doi.org/10.1097/MD.0000000000018766
- Romero Gómez M, González Pisano ME, Peñuela Avendaño O. Bilateral humeral head osteonecrosis. About a case. https://privada2023.secot.esvisor_posters_php.phpaccio=download&id=16385
- Banait S, Banait T, Shukla S, Mane S, Jain J. Bilateral Humeral Head Avascular Necrosis: A Rare Presentation in Sickle Cell Trait. Cureus. 2023; 15(8): e44006. https://doi.org/10.7759/cureus.44006
- Çavuş MC, Afacan MY, Zeytunlu A, Yapar A. Bilateral femur and humerus avascular necrosis associated with corticosteroids: A rare case presentation. Cureus. 2023; 15(12): e50834. https://doi.org/10.7759/cureus.50834
- Gómez-Mont Landerreche JG, Gil-Orbezo F, Morales-Domínguez H, Navarrete-Álvarez M, Trueba-Davalillo C, et al. Nontraumatic causes of bilateral avascular necrosis of the femoral head: Link between hepatitis C and pegylated interferon. Acta ortop. 2015; 29(3): 172-175. http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S2306-1022015000300006&lng=es
- Yassin M, Al-Mashdali AF, Al-Dubai HN. Avascular necrosis in patients with chronic myeloid leukemia: A systematic review. Acta Biomed. 2022; 93(1): e2022017. https://doi.org/10.23750/abm.v93i1.12270
- Kashkosh A, Peake CM, Narvani AA, Imam MA. Spontaneous avascular necrosis of the humeral head following COVID-19 vaccination. Arch Bone Jt Surg. 2023; 11(2): 140-143. https://doi.org/10.22038/ABJS.2022.67994.3243
- Agarwala S, Vijayvargiya M. Bisphosphonate combination therapy for non-femoral avascular necrosis. J Orthop Surg Res. 2019; 14(1): 112. https://doi.org/10.1186/s13018-019-1152-7