
Open Journal of Clinical and
Medical Images
Short Commentary - Open Access, Volume 2
Morphological anomalies of blood cells in COVID-19 patients
Giovanni Introcaso*; Maria Luisa Biondi
Unit of Laboratory Medicine, Centro Cardiologico IRCCS Monzino, Milan, Italy.
*Corresponding Author: Giovanni Introcaso
Unit of Laboratory Medicine, Centro Cardiologico IRCCS, Monzino, Via Parea, 20138 Milano, Italy.
Phone: 0039/0258002595
Email: giovanni.introcaso@ccfm.it
Received : Nov 01, 2022
Accepted : Dec 08, 2022
Published : Dec 16, 2022
Archived : www.jclinmedimages.org
Copyright : © Introcaso G (2022).
Abstract
Since March 2020, the laboratory’s workflow has been significantly modified and implemented to address the pandemic. Molecular as well as morphological features of blood cells are currenctly being investigated for the COVID-19 disease characterization. In the present study we aimed to show the morphological features of blood cells in COVID-19 patients. In the first and second waves, molecular diagnosis was carried out by Multiplex rRT-PCR from nasopharyngeal swabs. Currently, antigenic rapid test allows us to quicly screen patients on hospitalization. Hematochemical parameters were detected by XN 2000 hematology analyzer (Sysmex Corporation) and biochemical along with clinical data collected. A blood smear analysis using a May Grundwald Stain through a Leica ICC 50 HD microscope was performed. The abnormalities in the cell morphology were confirmed by biochemical and cytometric results. An analysis of leukocyte cell population data (CPD) demonstrated an association between the morphological features and the leukocyte CPDs (NE-SFL, LY-Y, MO-Y) showing an increase in cellular DNA/RNA content. C-reactive protein (CRP) and lactate dehydrogenase (LDH) were abnormal in every patient confirming an immunoinflammation state. We highlighted a wide morphological heterogeneity in the circulating blood cells of COVID-19 patients. Abnormalities were found in the leukocyte and platelet cell lines.
Keywords: Blood cells; COVID-19; Cellular anomalies.
Citation: Introcaso G, Biondi ML. Morphological anomalies of blood cells in COVID-19 patients. Open J Clin Med Images. 2022; 2(2): 1080.
Introduction
It is now well known that SARS CoV-2 infection causes multisystem abnormalities with hematologic disorders that can even lead to death.
Italy has been severely hit by the epidemic resulting in a great effort of health professionals. Several reports showed the clinical importance of blood quantitative and qualitative parameters [1,2]. Examination of the peripheral blood smear remains a key role for the haematological assessment. It was routinely used, to complete the analytical measurements and/or to evaluate the morphological features of blood cells often aiding to the diagnosis of hematologic or non-hematologic disorders. In our experience, hematologic parameters may aid to the COVID-19 diagnosis considering a careful analysis of cell blood count (CBC). An automated XN 2000 hematology analyzer (Sysmex Corporation) and a Leica ICC 50 HD microscope with a digital camera were used. Notably in the CBC assay, a limphopenia and a mild thrombocytopenia are associated to the first steps of viral infection [3,4]. In addition, leukocyte cell population data (CPD) were evaluted as optical signals indicating specific morpho-functional cell state [5]. Among different CPDs, NE-SFL (fluorescent light intensity of the neutrophil area on the WDF scattergram), LY-Y (fluorescent light intensity of lymphocyte) and MO-Y (fluores cent light intensity of monocyte) were selected as more significant. Previous studies, reported in COVID-19 cases reactive and plasmacytoid lymphocytes, platelet activation, significant left-shifted granulopoiesis with hypergranular, and vacuolated neutrophils or vacuolated monocytes [6]. Hereby, we describe several morphological cases of COVID-19 patients admitted to our cardiology hospital.

Description
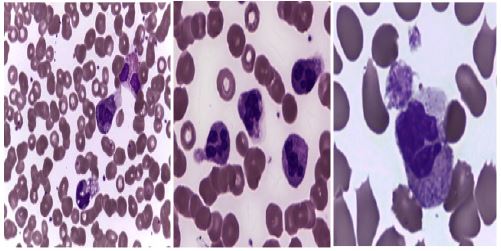
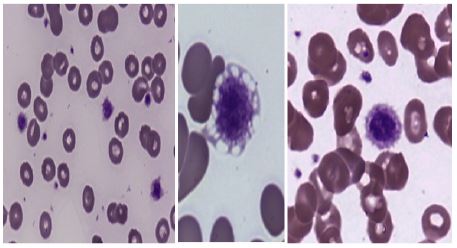
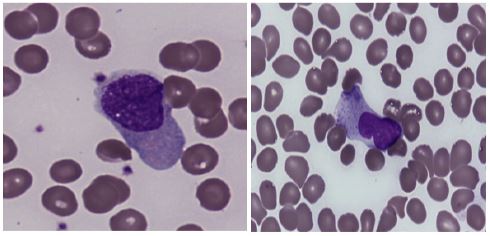
At the onset and progression of COVID-19 disease, blood cells are affected by significant functional and morphological changes. The present evaluation shows different features of leukocyte and platelet morphology, suggesting and immunoinflammation state due to Sars Cov-2 infection. The laboratory results confirmed those of the literature as a reduction of blood cells such as lymphopenia and thrombocytopenia associated with COVID-19 and its severity. Here, we illustrate blood films of several COVID-19 patients with different cellular activations in regard of leukocytes: granulocyte, lymphocyte, monocyte (Figures 1,2,4). Moreover, reticulated platelets or immature pletelet fraction (IPF) with activation are described (Figure 3). No morphological anomalies of erythrocytes were observed. In Image 1, upon activation reavealed by granulocyte ipergranulation, morphological changes are observed during the mechanism of NETosis, which is followed sometimes by cell rupture and subsequent cell death. These images demonstrate that neutrophils play a crucial role in immune-defense. In figure 2, we observed activated monocytes with multiple vacuoles. Of note, the presence of activated platelet in the same field. Similarly to neutrophil, but in the early phases of immuno response, monocytes are the first line of cellular adaptative response detecting the new viral antigens by specific receptor on the cellular membrane. Furthermore, the vacuoles suggest a cellular response even to possible bacterial superinfection that occurs in some COVID-19 severe diseases. The azurophilic cytoplasm of monocytes is indicative of increased DNA/RNA synthesis as a sign of high metabolic rate. In figure 3, platelets show more anomalies: large volume, hyperchromacy, different size with pseudopodia formation, vacuoles. These findings occurs both in patients with thrombocytosis and in those with thrombocytopenia [6]. Typically, in the early phases of viral infection, patients with mild thrombocytopenia may have a high immature platelet fraction (IPF) [4]. In fact, the reduction of platelet count may be the sentinel of the viral infection that signals endotheliopathy, leukocytes activation and the thrombo-inflammation state. In these COVID-19 patients, the platelets have the role of first immunological responders along with leukocytes. In Image 4, abnormalities of lymphocyte morphology are displayed. Of note, immature blast-like cells with reticular chromatin, basophilic cytoplasm and irregular nuclear shape. Similarly to monocytes, the increase of DNA/RNA synthesis suggests an intense metabolic activity, carrying out the function of antibody production.
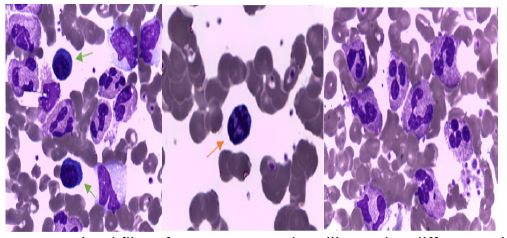
In figure 5, we show more cellular abnormalities in a same patient. He is a 66 year hold man affected by a severe COVID-19 illness with bilateral pneumonia. CBC was characterized by normal values except lymphopenia and an elevation of PLT count that becomes a thrombocytosis after illness evolution. The (orange) arrow indicates a picnotic lymphocyte; on the right, hypergranulated neutrophils and fragments of megakaryocytes. On the left, immature blast-like cells, monocytes and granulocytes, lymphocytes with clumped chromatin and deeply basophilic cytoplasm which are lymphoplasmocytoid cells are shown (green arrows).
Alterations of analytical leukocyte CPD, according to our morphological data, such as an elevation of NE-SFL, LY-Y and MO-Y values of light scattering (ch) compared to a reference population were found. In addition, biochemical markers confirmed the hematological derangements showing a significative immunoinflammation state. CRP and LDH had higher results compared to the laboratory cut-off: 5 mg/L and 225 UI/L respectively.
Discussion
From the first cases in 2020 of Sars Cov-2 infection, laboratory medicine with all the professions has stricly engaged. Consolidated data from the management of patients with COVID-19 suggest a multi-systemic involvement, including the hemopoietic system [1,2]. The involvement of leukocytes in the immune response, of monocytes and lymphocytes and recently platelets as immune and adaptive cells is known, however their pathophysiology in COVID-19 and their clinical application remains to be elucidated. Routine hematochemical assays of patients admitted to our hospital were used to characterize the disease. We enrolled some patients with molecular and clinical diagnosis of COVID-19 to evaluate the blood cell morphology gaining more information. In this investigation, we aimed to complete the hematochemical analysis such as CBC and cytometric results along with biochemical and clinical data. The morphological features of blood cells were illustrated as a heterogeneity of cellular components and structures that take place after viral infection. Here, we report many cellular alterations showing reactive changes in the circulating cells then in the hemopoietic system belonging to COVID-19 patients with a severe disease. Although data regarding the Net-osis do not have corresponded molecular finding, we showed the presence of extracellular traps of neutrophil morphologically. In other case, it was showed the activation of platelets and monocytes. Limphocytes activation was well described in term of increased cytoplasm/nuclear ratio, picnotic and lymphoplasmocytoid cells. These findings demostrated that Sars Cov-2 infection has the same charactestics as other viral infection with cytotoxic sequelae. These qualitative abnormalities may be related to the cytokine storm and hyperinflammation during the pathogenesis of the COVID-19 disease. In the anecdotal case (Figure 5), we presented a patient with many cellular anomalies that synthetise the clinical complications of a severe COVID-19. In this case, we have a complete hemopoiesis perturbation with alterations of granulocytes, lymphocytes and platelets at same time. In summary, it was pointed out that different cell morphological changes can be seen in different phases of COVID-19 and in different patients. Cellular alterations were confirmed by biochemical markers and by the leukocyte CPDs obtained from a hematology analizer.
Conclusion
Peripheral blood analysis offers valuable information in the diagnostic hematology process. Morphological assay may add information on the pathophysiology of COVID-19 disease and its progression. In this analysis, we confirm previous studies on hematologic abnormalities that occurs in patients affected by a severe viral pneumonia with clinical consequences that can ending in multi-organ failure. Moreover, the blood smear evaluation may detect in advance clinical manifestations in support of cytometric and biochemical data. Cellular anomalies or morphological indices could be useful for an automated learning process or a COVID-19 risk predictive model.
References
- Singh Rahi M., Jindal V., Reyes SP. et. al. Hematologic disorders associated with COVID-19: a review. Annals of Hematology. 2021; 100: 309–320
- Agbuduwe C, Basu S. Haematological manifestations of COVID-19. to coagulopathy. Eur J Haematol. 2020;105:540–546. https://doi.org/10.1111/ejh.13491
- Frater JL, Zini G, d’Onofrio G, Rogers HJ. COVID-19 and the clinical hematology laboratory. Int J Lab Hematol. 2020; 42(S1): 11-18.10.1111/ijlh.13229
- Introcaso G, Bonomi A, Salvini L, et. al. High immature platelet fraction with reduced platelet count on hospital admission. Can it be useful for COVID-19 diagnosis? Int J Lab Hematol. 2021; 00: 1–6.
- Diagnostic and prognostic utility of WBC counts and cell population data in patients with COVID-19. Int J Lab Hematol. 2021; 43(Suppl. 1): 124–128.
- Zini G, Bellesi S, Ramundo F, d’Onofrio G. Morphological anomalies of circulating blood cells in COVID-19. Am J Hematol. 2020; 95(7): 870-872.