
Open Journal of Clinical and
Medical Images
Research Article - Open Access, Volume 3
Macroglossia as the first clinical manifestation of
systemic amyloidosis associated with multiple
myeloma and a literature review
Xiuzhen Wen1,2; Zhihui Liu1; Xiongyan Luo1; Yi Liu1*
1Department of Rheumatology and Immunology, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, China.
2Department of Rheumatology and Immunology, Jiujiang NO.1 People’s Hospital, 48 South Taling Road Jiujiang 332000, Jiangxi province, China.
*Corresponding Author: Yi Liu
Department of Rheumatology and Immunology, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, China.
Email: yiliu8999@wchscu.cn
Received : Dec 07, 2022
Accepted : Jan 10, 2023
Published : Jan 17, 2023
Archived : www.jclinmedimages.org
Copyright : © Liu Y (2023).
Abstract
Objective: To report a case of systemic amyloidosis manifested as macroglossia and summarize review its current literature.
Methods: First, we retrieved patient’s disease data from the West China Hospital, Sichuan University, electronic medical record system. For the literature review, we searched Cochrane, Web of Science, PubMed, and EMBASE for relevant articles published from January 1, 1947, to December 31, 2020.
Results: A 43-year-old Chinese Han female patient was presented with tongue painless progressive enlargement. The tongue biopsy showed amyloid by Congo red staining, and the bone marrow aspiration revealed a large clonal plasma cells’ number (39%). The systematic examination results revealed extremities thickened skin. The patient was diagnosed with systemic lambda light chain amyloidosis associated with multiple myeloma and received cyclophosphamide combined with bortezomib and dexamethasone. During the 8-month follow-up, symptoms were relieved without recurrence. We found 12 reports describing 19 Amyloid light-chain (AL) amyloidosis patients with multiple myeloma (11 females, 57.89%) in the literature search. The first symptom was macroglossia in all patients. Detailed immunoglobulin light chain analysis was performed in nine patients, with lambda being predominant.
Conclusion: Systemic AL amyloidosis with macroglossia is often associated with multiple myeloma occurrence, and its clinical prognosis is extremely poor. Also, it can be a multiple myeloma paraneoplastic phenomenon and should be watched in clinical practice.
Keywords: Macroglossia; Systemic amyloidosis; Immunoglobulin light chain; Multiple myeloma; Paraneoplastic.
Clinical practice points
• Macroglossia as initial clinical presentation in systemic amyloidosis is rare.
• We report a case of systemic AL amyloidosis characterized by painless progressive tongue enlargement.
• Systemic AL with macroglossia as a clinical manifestation was associated with MM and clinicians should be aware of it.
Citation: Wen X, Liu Z, Luo X, Liu Y. Macroglossia as the first clinical manifestation of systemic amyloidosis associated with multiple myeloma and a literature review. Open J Clin Med Images. 2023; 3(1): 1088.
Introduction
Systemic amyloidosis comprehends a group of rare diseases caused by misfolded proteins deposition outside tissue cells, leading to multiple organ dysfunction, failure, and even death [1]. According to the precursor protein type, amyloidosis can be divided into immunoglobulin light chain, amyloid protein A, transthyroxine protein, apolipoprotein A-I, and lysozyme types [2]. Among them, systemic light-chain (AL) amyloidosis is the most common, accounting for 55-65% of all cases in the UK and even 93% in Chinese amyloidosis patients [3,4].
AL amyloidosis is associated with clonal plasma cell proliferative disorders - the amyloid material being formed by misfolding of monoclonal immunoglobulin light chains [3,5]. This amyloidosis tends to occur in middle-aged and elderly patients, the male/female ratio is about 2-3:1, and the median survival time is 36.3 months. Diagnosis is often based on clinical manifestations combined with pathological biopsy [3]. Relevant tissue biopsies should be performed as soon as amyloidosis is highly suspected clinically.
Systemic AL amyloidosis is clinically heterogeneous and often involves organ systems such as kidneys, heart, gastrointestinal tract, liver and spleen, and peripheral nerves, with rare tongue cases as well [1,3]. The classic amyloid deposition manifestation in the oral cavity is macroglossia or buccal mucosa nodular hyperplasia, and, once present, is often instructive for diagnosis [1]. A previous study has shown that the presence of Multiple Myeloma (MM) accounted for 15% of AL amyloidosis patients [6]. However, systemic amyloidosis with MM in which macroglossia is the initial clinical feature is very rare in clinical practice. In this study, we reported a patient with macroglossia as the first manifestation, in whom AL amyloidosis combined with MM was considered for diagnosis. Finally, we also conducted a literature review on this matter.
Materials & Methods
The patient’s medical records, including history, physical examination, and laboratory tests were collected. A biopsy of the tongue was obtained and stained with Hematoxylin-Eosin and Congo red. We also searched Cochrane, Web of Science, PubMed, and EMBASE for relevant articles published from January 1, 1947, to December 31, 2020. The following terms were used in the literature search: “tongue” and “amyloidosis” and “myeloma multiple”, “Plasma Cell Myelomas”, “Myelomatoses”, “Myelomatosis” “Plasma-Cell Myelomas”. The inclusion criteria for this literature review include English case reports and case series published between January 1947, and December 2020, reporting information on systemic amyloidosis with MM with macroglossia as the first clinical manifestation. We excluded articles about limitations and secondary amyloidosis case studies. According to requirements, we obtained written informed consent from the patient included in this study.
Results
Case presentation
A 43-year-old Chinese Han female present to our hospital complaining tongue painless progressive enlargement that had appeared 2 years ago. The patient had been surgically treated with resection in a local hospital in 2018 but recurred in 2019. Since 2019, the patient presented progressive tongue mass growth with difficulties extending her tongue, occasional lower limb acid swelling discomfort, and had lower limb numbness discomfort at night. She did not report any alterations in appetite, sleeping, or weight.
The patient was neither a smoker nor a drinker and her medical history was unremarkable. Regarding first-degree relatives, the patient’s eldest sister had thyroid cancer, and the second had passed away due to a bladder tumor. However, other relatives, including parents, were healthy.
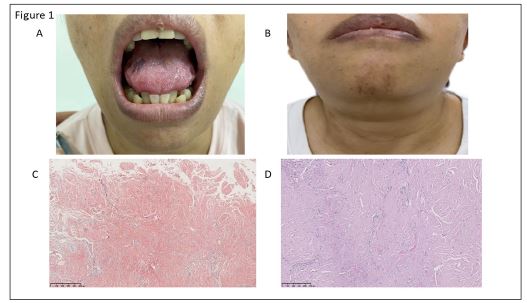
Physical examinations revealed an enlarged tongue with visible swelling around the lip (Figure 1A and B). Multiple masses were palpable submandibular with indistinct borders, hard and without significant tenderness. Multiple enlarged lymph nodes were palpable in the axillae bilaterally, and the extremities’ skin was tight.
Her blood routine and liver and kidney function tests were within normal ranges. Blood immunofixation electrophoresis showed that the λ light chain M protein was positive, urine λ light chain was 9.85 g/L, and urine κ light chain was 0.0449 g/L. Bone marrow aspiration showed clonal plasma cells that accounted for 39%, and immunophenotyping showed infiltrating plasmacytoid cells CD38 (+), CD138 (-), CD56 (-), Ig κ (-), and Ig γ (+). Eosinophilic material deposits, within the muscle fibers and interstitium, few hyperplastic fibroblasts and positive Congo red staining were seen on the tongue biopsy (Figure 1C and D). Therefore, amyloidosis was considered.
Finally, the patient was diagnosed with AL amyloidosis associated with MM. Then, she received cyclophosphamide (0.4 g/week), bortezomib (1.3 mg/week), and dexamethasone (15 mg twice a week) combined treatment. During the 8-month follow-up, her tongue was smaller and the clinical symptoms improved.
Literature review of macroglossia as the first symptom of systemic amyloidosis complicating MM.
We screened 1782 articles in this literature review, and only 12 were eligible (Table 1). We found 19 relevant cases, including the one that we reported in this study. Among the 19 patients, 8 (42.11%) were male and 11 (57.89%) female. The mean patients’ age was 66.13 years for males and 69.7 years for females. Disease duration ranged from 1-60 months. The most frequently reported countries were the United States and the Netherlands (four patients each), followed by Israel (2), India (1), Chile (1), Brazil (1), Ireland (1), Turkey (1), and China (1).
Bone marrow aspiration was performed in all patients. Seventeen had a tongue biopsy, and one had a renal biopsy. One died quickly and did not have a tongue biopsy. All patients with tongue biopsy showed positive Congo red staining. Immunohistochemical analysis was performed in 11 cases, and the light chain type was reported in nine of them (five with λ, three with κ, and one with both λ and κ). In the remaining two cases, only the light chain protein presence was reported, without specific typing analysis. Most patients (18/19) had MM, and, in 11/19 cases, the Bence-Jones protein was found in blood or urine.
Table 1: Literature review.
| Years | Disease duration course | Sex | Age | Nation region | Bence-Jones protein | Light chain | Other organs and presentations involved | Therapeutic regimen treatments | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| month | |||||||||
| 1947 [7] | 18 | M | 72 | US | + | NA | NA | NA | NA |
| 60 | M | 63 | US | — | NA | NA | NA | NA | |
| 1957 [8] | NA | F | 60 | NA | + | NA | Joint | NA | Death |
| NA | F | 68 | NA | + | NA | NAe | NA | Death | |
| 1985 [9] | 2 | F | 75 | NA | + | κ | Heart | CTX, MP | Death |
| 1990 [10] | 3 | F | 55 | India | + | k | Kidney, Joint | Melphalan | Death |
| 1994 [11] | NA | M | 65 | US | + | κ | NA | NA | NA |
| 2002 [12] | NA | F | 80 | Netherlands | NA | λ | Skin, | Chemotherapy | Death |
| Heart | |||||||||
| NA | F | 77 | Netherlands | NA | λ | Heart, | Chemotherapy | Death | |
| Intestinum tenue | |||||||||
| NA | F | 73 | Netherlands | NA | λ | Heart, | Chemotherapy | Death | |
| Skin | |||||||||
| 2005 [13] | NA | M | 69 | Ireland | + | NA | NA | Melphalin and prednisone | Death |
| 2010 [14] | 9 | M | 62 | Israel | + | κ | Skin, | bone marrow transplantation | Death |
| Nerves, Kidneys | |||||||||
| 36 | M | 65 | Israel | + | κ, λ | Digestive tract | surgical resection | Death | |
| 2017 [15] | 6 | F | 54 | Turkey | NA | NA | Kidney | Chemotherapy | Death |
| 2018 [16] | 12 | M | 75 | Brazil | + | NA | Nerve | NA | Death |
| 2018 [17] | 1 | F | 73 | Chile | + | NA | Kidney | Hemodialysis, chemotherapy | Death |
| 2018 [18] | NA | M | 58 | US | + | λ | Heart | Botizomide, lenamide dexamethasone, AHSCT | Improve |
| 2020(Our’s) | 24 | F | 43 | China | + | λ | None | Bortezomib, CTX | Improve |
In all reported cases, in addition to tongue involvement, other organs were involved including the heart (5), kidney (3), gastrointestinal tract (3), skin (2), muscles (1), and joints (1). Ten patients received chemotherapy, 1 received dialysis treatment combined with chemotherapy, 1 received surgery, and 1 received bone marrow transplantation. However, in 3 cases, the treatment regimen and prognosis were not reported. Finally, only 2 patients died during the follow-up.
Discussion
AL amyloidosis is the most common systemic amyloidosis and its clinical presentations are highly heterogeneous and largely depend on the organs affected. Compared with the heart and kidneys, soft tissues (e.g. tongue) are less affected.
The most common amyloid deposition site in the oral cavity is the tongue, and typical manifestations usually include yellow changes, papules, nodules, plaques, and macroglossia [12]. The case described in this study is mainly characterized by painless tongue enlargement, and tongue amyloidosis combined with MM.
A previous study has shown that 21% (4/191) of AL amyloidosis and MM patients developed macroglossia [19]. Nevertheless, there are few studies on tongue manifestations of AL combined with MM. Therefore, we reviewed studies with AL patients combined with MM using macroglossia as the initial clinical manifestation and mainly found case reports. In our review, λ was the main light chain type among AL-MM patients with macroglossia as the first manifestation, and most clinical outcomes were not good. These suggested that complete examinations such as bone marrow puncture and tongue biopsy should be performed as soon as possible in those patients, to not delay MM diagnosis and treatment.
Tongue amyloidosis might be regarded as a plasma cell malignancy paraneoplastic phenomenon [12]. A previous study found that 7 of 11 patients with oral (tongue and oral mucosa) amyloidosis were diagnosed with MM and that 3 patients had monoclonal gammopathy of undetermined significance [12]. Also, Xu et al. studied 158 patients with MM and found that AL amyloidosis was a poor independent prognostic factor [20]. In this study, 31% (49/158) of patients were diagnosed with AL amyloidosis. The main organs involved were the kidney (36, 73.4%) and the heart (27, 55.1%). At the same time, the survival time of MM with amyloidosis was significantly shorter compared to patients only with MM.
In our study, AL amyloidosis immunoglobulin light chains were dominated by λ light chains. A previous study has reported that in AL amyloidosis, λ immunoglobulin light chain was produced in 80% of cases and κ in the remaining 20% [21]. Also, another study has shown that the λ light chain was predominant in AL amyloidosis patients [22]. In MM, the λ type appears more than the κ type, and one study suggested that λ type MM can be an AL amyloidosis high-risk factor in the disease course [20]. This can be attributed to a greater λ chain "amyloidosis" and an imbalance in the speed of light chain removal and deposition [22,23]. However, liver involvement and severe renal impairment were more frequently found in κ amyloidosis than in λ [24] Moreover, the incidence of AL amyloidosis in κ type MM was lower but more severe compared to λ MM [25].
Conclusion
Compared with the heart and kidneys, tongue amyloid involvement is rare and does not often attract attention from clinicians. However, in our study, systemic amyloidosis with macroglossia as the first clinical manifestation was mostly complicated by MM (18/19) and had poor outcomes. Mega tongue-like systemic amyloidosis is not frequently considered first as systemic amyloidosis or MM in clinical practice. Diagnosis can only be confirmed when the disease progress to late stages, likely causing irreversible consequences. Therefore, we hope that our research will improve the understanding of patients with macroglossia as the first manifestation, and enhance the use of complete tongue biopsy and bone marrow aspiration, as well as the screening of serum protein electrophoresis or urine Bence-Jones protein, to achieve early diagnosis and intervention.
Disclosure: The authors have stated that they have no conflicts of interest.
References
- Merlini G, Dispenzieri A, Sanchorawala V, Schönland SO, Palladini G, et al. Systemic immunoglobulin light chain amyloidosis. Nat Rev Dis Primers. 2018; 4: 38.
- Perfetto F, Moggi-Pignone A, Livi R, Tempestini A, Bergesio F, et al. Systemic amyloidosis: a challenge for the rheumatologist. Nat Rev Rheumatol. 2010; 6: 417-429.
- Huang XH, Liu ZH. The Clinical Presentation and Management of Systemic Light-Chain Amyloidosis in China. Kidney Dis (Basel). 2016; 2: 1-9.
- Ravichandran S, Lachmann HJ, Wechalekar AD. Epidemiologic and Survival Trends in Amyloidosis, 1987-2019. N Engl J Med. 2020; 382: 1567-1568.
- Pratt G. Bortezomib, Melphalan, Dexamethasone: A New Standard of Care for AL Amyloidosis? J Clin Oncol. 2020; 38: 3243-3244.
- Ebert EC, Nagar M. Gastrointestinal manifestations of amyloidosis. Am J Gastroenterol. 2008; 103: 776-787.
- BRUNSTING LA, MacDONALD ID. Primary systematized amyloidosis with macroglossia; a syndrome related to Bence-Jones proteinuria and myeloma. J Invest Dermatol 1947; 8: 145-165.
- CAHN L. Oral amyloid as a complication of myelomatosis. Oral Surg Oral Med Oral Pathol. 1957; 10: 735-742.
- Babajews A. Occult multiple myeloma associated with amyloid of the tongue. Br J Oral Maxillofac Surg. 1985; 23: 298-303.
- Loh FC, Ravindranathan N, Yeo JF. Amyloidosis with oral involvement. Case report. Aust Dent J. 1990; 35: 14-18.
- Reinish EI, Raviv M, Srolovitz H, Gornitsky M. Tongue, primary amyloidosis, and multiple myeloma. Oral Surg Oral Med Oral Pathol. 1994; 77: 121-125.
- van der Waal RI, van de Scheur MR, Huijgens PC, Starink TM,. Amyloidosis of the tongue as a paraneoplastic marker of plasma cell dyscrasia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94: 444-447.
- Kelly M, Moran J. Macroglossia and carpal tunnel syndrome associated with multiple myeloma: a case report. Ir J Med Sci. 2005; 174: 95-96.
- Elad S, Czerninski R, Fischman S, Keshet N, Drucker S,. Exceptional oral manifestations of amyloid light chain protein (AL) systemic amyloidosis. Amyloid 2010; 17: 27-31.
- Demirkan S, Şavk E, Alp A. Macroglossia as a presenting feature of multiple myeloma. J Family Med Prim Care. 2017; 6: 146-147.
- da Costa KVT, Ribeiro CMB, de Carvalho Ferreira D, et al. Dysphagia due to macroglossia in a patient with amyloidosis associated with multiple myeloma: A case report. Spec Care Dentist. 2018; 38: 255-258.
- Maturana-Ramírez A, Ortega AV, Labbé FC, de Moraes Ê, Aitken-Saavedra JP. Macroglossia, the first manifestation of systemic amyloidosis associated with multiple myeloma: Case report. J Stomatol Oral Maxillofac Surg. 2018; 119: 514-517.
- Williams MU, Murphy CE, Gore RS, Fentanes E. Lingual liability: macroglossia and dyspnoea as the harbinger of systemic AL (light-chain) cardiac amyloidosis. BMJ Case Rep. 2018; 11: e225923.
- Flores-Bozo LR, Echevarría-Keel J, Domínguez-Cherit J, Esquivel-Pedraza L, Méndez-Flores S. Mucocutaneous manifestations in systemic amyloidosis A retrospective analytical study in a tertiary care center. Int J Dermatol. 2019; 58: 1062-1068.
- Xu J, Wang M, Shen Y, Yan M, Xie W. Effects of Amyloid Light-Chain Amyloidosis on Clinical Characteristics and Prognosis in Multiple Myeloma: A Single-Center Retrospective Study. Cancer Manag Res. 2021; 13: 1343-1356.
- Sidana S, Tandon N, Dispenzieri A, Gertz MA, Buadi FK, et al. Clinical presentation and outcomes in light chain amyloidosis patients with non-evaluable serum free light chains. Leukemia. 2018; 32: 729-735.
- Solomon A, Weiss DT, Kattine AA. Nephrotoxic potential of Bence Jones proteins. N Engl J Med. 1991; 324: 1845-1851.
- Desikan KR, Dhodapkar MV, Hough A, Waldron T, Jagannath S. Incidence and impact of light chain associated (AL) amyloidosis on the prognosis of patients with multiple myeloma treated with autologous transplantation. Leuk Lymphoma. 1997; 27: 315-319.
- Huang X, Wang Q, Jiang S, Chen W, Zeng C. The clinical features and outcomes of systemic AL amyloidosis: a cohort of 231 Chinese patients. Clin Kidney J. 2015; 8: 120-126.
- Sidiqi MH, Aljama MA, Muchtar E, Zeng C, Liu Z. Light chain type predicts organ involvement and survival in AL amyloidosis patients receiving stem cell transplantation. Blood Adv. 2018; 2: 769-776.