
Open Journal of Clinical and
Medical Images
Clinical Image - Open Access, Volume 3
Esophageal plexiform fibromyxoma: An unusual localization
Lorenzo Del Nero1*; Sebastiano Ziola1; Anna Dellachà2; Paolo Quilici2; Antonella De Ceglie3*; Massimo Conio1
1S.C. Gastroenterologia ASL 2 Savonese, Ospedale Santa Corona, Pietra L. (SV), Italy.
2S.C. Anatomia Patologica ASL 2 Savonese, Ospedale Santa Corona, Pietra L. (SV), Italy.
3S.S.D. Gastroenterologia ASL 1 Imperiese, Ospedale Civile di Sanremo (IM), Italy.
*Corresponding Author: Lorenzo Del Nero
S.C. Gastroenterologia ASL 2 Savonese, Ospedale Santa Corona, Pietra L. (SV), Italy.
Email: l.delnero@asl2.liguria.it
Received : Mar 06, 2023
Accepted : Apr 14, 2023
Published : Apr 21, 2023
Archived : www.jclinmedimages.org
Copyright : © Del Nero L (2023).
Citation: Del Nero L, Ziola S, Dellachà A, Quilici P, Ceglie A, et al. Esophageal plexiform fibromyxoma: An unusuallocalization. Open J Clin Med Images. 2023; 3(1): 1106.
Introduction
Plexiform Fibromyxoma (PF) is an infrequent mesenchymal tumor of the Gastrointestinal Tract (GI). The reported incidence of PF relative to GI Stromal Tumor (GIST) is estimated 1.7% over a time of 20 year [1].
PF is mostly found in the gastric antrum. However, it has been described in other GI tract segments such as duodenum, jejunum, gallbladder and mediastinum [2]. Esophageal presentation is extremely rare.
A case report of an esophageal PF is described in a 55-year-old woman.
Case report
A 55-year-old woman with a two-year history of mild dysphagia was referred to our Endoscopy Center for evaluation of a proximal esophageal polyp found in a previous esophagogastroduodenoscopy.
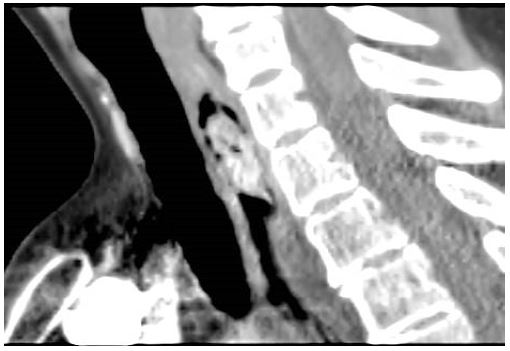
A CT scan of the neck revealed thickening of the cervical esophagus in the absence of other pathological finding (Figure 1).
An endoscopic re-evaluation confirmed a 30 mm sessile polyp with high vascularity. Endoscopic Submucosal Dissection (ESD) of the lesion was performed without immediate or late adverse events.
Macroscopic examination revealed a 3.1 x 2.6 cm lesion with a bozzellated and partly hemorrhagic surface.
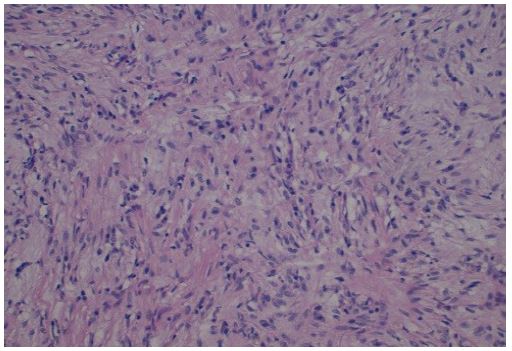
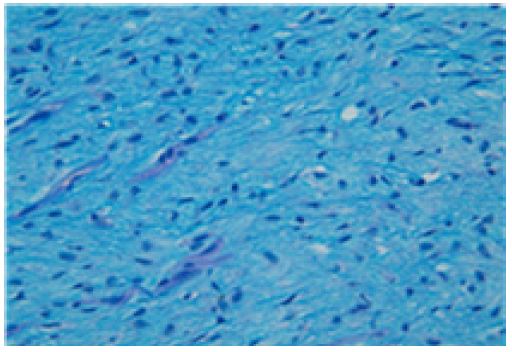
The pathological features were: a multinodular proliferative lesion, composed of bland, uniform spindle-ovoid cells with no mitotic activity, in richly vascularized interstizial mixoid matrix with focal chronic inflammatory chances. The proliferative index (MIB1/Ki67) was 1%. Immunohistochemistry: neoplastic cells express smooth muscle actin. S100, H caldesmon, CD117, DOG1, CD34, SOX10, CKAE1-AE3 GFAP, MUC4, MDM2 were negative (Figure 2, Figure 3, Figure 4).
Strikingly the histo-cytopathological analysis led to diagnosis of plexiform fibromyxoma.

Discussion
Due to its rarity, not many cases of PF have been described in literature. In particular, esophageal presentation is extremely rare.
Pathogenesis and molecular alterations of PF are largely unknown and its incidence seems to be increasing in the last years [3].
PF is equally described in males and females and the median age at presentation is 40 years to 50 years, although pediatric cases have been described as well [4,5].
In the majority of patients, the clinical presentation is not specific: abdominal pain, early fullness, vomiting and anemia are sometimes present.
Due to the submucosal localization of the tumor, EUS + FNA are considered the diagnostic gold standards, even if primary resection is usually the first choice [6].
The pathologist's approach to gastroesophageal mesenchymal tumours has been deeply reviewed in the last years thanks to increasingly detailed genetic subclassification. Specific treatments optimized for particular genetic subtypes are now available [7].
PF are usually considered benign conditions, even if vascular, lymphatic and mucosal invasion have been described. Neoplasia with similar histologic features (GIST, smooth muscle tumors) have instead a malignant potential [1]. For this reason, an accurate differential diagnosis is essential [6].
References
- Arslan ME, Li H, Jennings TA, Lee EC, Nigam A, et al. Frequency of Plexiform Fibromyxoma relative to gastrointestinal stromal tumor: A single center study. Ann Diagn Pathol. 2020; 48: 151568.
- Arslan ME, Li H, Fu Z, Jennings TA, Lee H. Plexiform fibromyxoma: Review of rare mesenchymal gastric neoplasm and its differential diagnosis. World J Gastrointest Oncol. 2021; 13: 409-423.
- Takahashi Y , Suzuki M, Fukusato T. Plexiform angiomyxoid myofibroblastic tumor of the stomach. World J Gastroenterol. 2010; 16: 2835-2840.
- Su HA, Yen HH, Chen CJ. An Update on Clinicopathological and Molecular Features of Plexiform Fibromyxoma. Can J Gastroenterol Hepatol. 2019; 2019: 3960920.
- Duckworth LV, Gonzalez RS, Martelli M, Liu C, Coffin CM, et al. Plexiform fibromyxoma: report of two pediatric cases and review of the literature. Pediatr Dev Pathol. 2014; 17: 21-7.
- Magadán Álvarez C, Olmos-Martínez JM, Toledo Martínez E, Trugeda Carrera MS, Fernández Díaz MJ, et al. Gastric plexiform fibromyxoma, an uncommon mesenchymal tumor. Rev Esp Enferm Dig. 2021; 113: 183-185.
- Papke DJ Jr, Hornick JL. Recent developments in gastroesophageal mesenchymal tumours. Histopathology. 2021; 78: 171-186.