
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 3
Laser excision of congenital epulis in an one-year-old infant: A case report with 6-months follow-up
Agrawal AA1*; Patil VR2
1Department of Periodontics, MGV’s KBH Dental College and Hospital, Panchvati, Nasik -422003, MHS, India.
2Pediatric Dentistry, Private Practioner and consultant, Nasik, MHS, India.
*Corresponding Author: Agrawal AA
Department of Periodontics, MGV’s KBH Dental College and Hospital, Panchvati, Nasik -422003, MHS, India.
Email: agrodent@rediffmail.com
Received : Apr 24, 2023
Accepted : Jun 01, 2023
Published : Jun 07, 2023
Archived : www.jclinmedimages.org
Copyright : © Agrawal AA (2023).
Abstract
Congenital epulis are present at birth and might maintain the same size or grow slowly. They are more often reported within first month after birth are more commonly reported in female infants. In this article, a rare instance of a congenital giant cell fibroma in a male infant is described, who reported to consulting after one year of age. During clinical examination, tissue growth was detected on the right maxillary anterior alveolar ridge area, which was supposedly interfering the growth of underlying deciduous tooth. Management of case involved the use of a diode laser to excise the fibroma under local anaesthesia. Follow-up visit after 6-months showed excellent healing which also facilitated eruption of underlying deciduous tooth (#53). The article also emphasizes the significance of proper oral examination beginning in infancy for clinicians to make early diagnoses and provide more effective treatments for oral disorders, as well as promote better oral health in the community.
Citation: Agrawal AA, Patil VR. Laser excision of congenital epulis in an one-year-old infant: A case report with 6-months follow-up. Open J Clin Med Images. 2023; 3(1): 1110.
Introduction
Neumann in 1871 [1] coined the term ‘congenital epulis’ which he described as a circumscribed soft-tissue swelling on the alveolar ridge of new-born infants. The most obvious striking feature is that they are present at birth and might maintain the same size or grow slowly over next few months or years (if not treated). Majority of these congenital epulis are present in maxilla but they have been reported in both the jaws. The most common location being anterior region. Their size can vary from few millimetres to as large as 9 cm, causing difficulty in breathing and feeding. They are slow growing and have a good success rate after excision. Unlike the present case, congenital epulis are more frequently seen in female infants. All forty cases reported by Custer and Fust [2] were female infants. Claim by Lange [3] that it occurs eight time more frequently in girls than boys also supports the data.
Histologically congenital epulis resembles granular-cell myoblastoma, so much so that some workers believed them to be the same lesion. However, in contrast to the later, psudoepitheliomatous hyperplasia of the overlying surface epithelium is not a common finding in congenital epulis. Other lesions such as gingival cyst of new-born, vascular malformations, cystic higroma, melanotic neuroectodermal tumor of infancy, oral teratoma and malignant tumors such as the rhybdomyosarcoma can be clinically similar to the congenital epulis but their clinical behaviour and histological aspects are diagnostically different.
Congenital epulis is still considered a clinical rarity. In a review of cases over a 50-year (period: 1907-1957), Pape and Hawkins [4] encountered only one case of congenital epulis. Similarly, records of cases seen by Kong-Wing and Yeow CS [5] over a period of 22 years (1949 to 1971) found only two cases of congenital epulis.
Surgical removal can be accomplished with a standard scalpel, electrosurgery, infrared lasers (diodes, erbium, neodymium, and CO2), or cryosurgery. When comparing these options, the laser provides the best postoperative phase and certain advantages, as indicated by Bornstein et al [9] and Rossmann et al [6].
1. The rapid ablation of soft tissue, including lymphatic and blood arteries, results in appropriate sealing, which supports exact removal of the pathology and improves visibility of the operative area.
2. Minimum contact with pathological tissues.
3. Due to Laser sterilization, risk of infection is reduced.
4. It greatly lowers pain, inflammation, and postoperative infections, while also closing nerve terminals.
5. Less wound contraction, favouring the absence of scars.
6. Less injury to nearby tissues (without altering the surface of implants and under the prescribed settings and protocols, not affecting the dental pulp).
7. Less use of anaesthetics and less or no need for sutures.
8. Less use of analgesics and antibiotics.
In short, the laser promotes faster healing and a healthier postoperative phase. Equipment costs, adherence to strict safety rules, such as the usage of required lenses, and training in the administration of this new technology are some of the drawbacks of laser use [6,7].
Case study
Parents of a one-year-old boy reported in a paediatric dentist consultation with a complaint of a soft tissue enlargement on the right maxillary anterior ridge of the boy. A clinical examination of the infant revealed no additional oral swelling or deformity, however the localized enlargement seemed to hamper the eruption of underlying deciduous tooth. An intraoral examination revealed a sessile soft tissue nodule measuring 1.3 cm x 0.6 cm on the vestibule extending to the maxillary ridge distal to the upper right primary incisor teeth. The lesion was non-hemorrhagic, non-tender on palpation, and covered by intact white mucosa (Figure 1). A clinical diagnosis of epulis was made, topical anesthesia then the infiltration of Lignocaine (1:200000, 30-gauge ½” needle) was given and an excisional biopsy was done with a diode laser (Picasso, USA- 840 nm, power settings of 2.5-Watt, intermittent mode, and a tip diameter of 300 microns) (Figure 2).
According to the protocol, excised tissue was sent for histopathological examination. The surgery was completely bloodless following basic oral health counselling, and the infant was discharged after analgesics were prescribed.
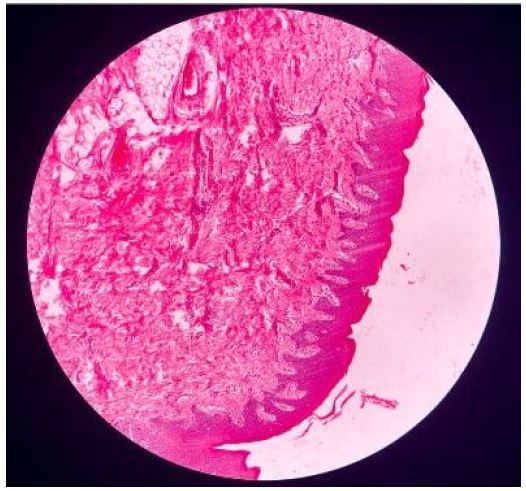
The histopathological report revealed ulcerated stratified squamous epithelium with short rete pegs around the connective tissue stroma with numerous collagen fiber bundles, proliferating spindle-shaped fibroblasts with mild chronic inflammatory cell infiltration, mature adipocytes at the periphery (Figure 3). Overall, the histological findings were suggestive of fibroma.
The patient was recalled after 24 hours for immediate follow-up. The excised area was whitish in color. The patient was calm and comfortable. Parents reported that the infant had good sleep and he was feeding comfortably. The patient was recalled after 15-days again for evaluation of the wound site.



At the 1-month follow up the wound site satisfactorily healed and the tip of tooth #53 (right maxillary deciduous canine) was seen at the crest of the alveolar ridge. The patient and parent both seemed happy and satisfied. Parents were advised to visit again after 3-months for follow-up. Patient skipped the next appointment and reported directly at 6th-month post-surgery. At this time, the tooth #53 was completely erupted and the healing was good as shown in Figure 4. Parents were given oral hygiene instruction and advice to routine follow-up visits every 6 months henceforth.
Discussion
This article described a congenital fibroma on the anterior region of maxillary ridge distal to the upper right primary incisors in an infant.
The widely accepted hypothesis regarding the cause of congenital epulis is that they are derived from primitive mesenchymal cells that have been submitted to molecular and cytoplasmic transformations, resulting from epigenetic factors [10]. In contrast to the current case where patient was almost an year old male infant, majority of reports of congenital epulis are of patients reporting from 7-days post birth to 30-days after birth. A recent case report by Bernaola-Paredes et al [11] in 30-day old female infant was treated with diode laser and was very safe and effective.
The safety and efficacy of diode laser systems have been widely demonstrated in the treatment of vascular lesions, fibromas, gingival hyperplasia, and epulis. Dental lasers provide therapeutic benefits such as reduced bleeding and anaesthetic requirements, as well as reduced postoperative discomfort and inflammation owing to the sealing of blood and lymphatic vessels. Furthermore, because of their bactericidal activities, the probability of infection is reduced as compared to traditional surgery [12], they induce less scar tissue contraction and retain the elastic qualities of tissues [13,14]. The diode laser has gained a lot of popularity in dentistry due to its portability and simplicity of use for soft tissues in minor surgeries. Fibroma has no potential to become malignant, and after complete excision, recurrence is uncommon.
Even though they are common lesions of the oral cavity and have distinct features, fibromas can occasionally be difficult to diagnose. For the diagnosis to be confirmed and for such instances to be managed appropriately, a thorough history of the lesion, accurate clinical evaluation, and microscopic examinations are needed. Correct diagnosis and treatment avoids trouble in the development of the jaws in children due to its possibility or getting large in size and its critical location. Its clinical appearance usually causes anxiety in parents and after its removal the healing is uneventful and also helps in physiologic and psychological development of the child.
Conclusion
Several fibrous hyperplastic lesions are clinically and histologically similar, to make an accurate diagnosis, a biopsy is necessary. According to the diode laser use regulations, its relative simplicity and high level of safety can produce good results.
References
- Neumann E. Ein Fall von congenitaler Epulis, Arch Heilkd. 1871; 12: 189.
- Custer RP, Fust JA. Congenital Epulis. Am J Clin Pathol. 1952; 22: 1044.
- Lange D. Morphology and Histogenesis of Congenital Epulides. Dent Abstr. 1964; 105.
- Pape TJ, Hawkins DB. Congenital Granular-Cell Myoblastoma of the Oral Cavity. Oral Surg. 1962; 15: 377.
- King-Wing Y, Yeow CS. A congenital peripheral ossifying fibroma. Oral Surg. 1973; 35: 661-666.
- Rossmann JA. Reactive lesions of the gingiva: diagnosis and treatment options. The Open Pathology Journal. 2011; 5: 23-32.
- Bornstein MM, Winzap-Kälin C, Cochran DL, Buser D. The CO2 laser for excisional biopsies of oral lesions: a case series study. Int J Periodontics Restorative Dent. 2005; 25: 221-229.
- Rossmann JA, Cobb CM. Lasers in periodontal therapy. Periodontology 2000. 1995; 9: 150-164.
- Shalawe WS, Ibrahim ZA, Sulaiman AD. Clinical comparison between diode laser and scalpel incisions in oral soft tissue biopsy. Al-Rafidain Dent J. 2012; 12: 337-43.
- Kokubun K, Matsuzaka K, Akashi Y, Sumi M, Nakajima K, Murakami S, et al. Congenital epulis: A case and review of the literature. Bull Tokyo Dent Coll. 2018; 59: 127‑132.
- Bernaola‑Paredes WE, Conceição MB, Moreira SC, Souza AM, Pina PS, et al. Clinical and histopathological features of congenital epulis in a newborn submitted to laser surgery. J Oral Maxillofac Pathol. 2022; 26: S77-9.12.
- Desiate A, Cantone S, Profeta G, Grassi F R, Ballini A, Tullo D. 980nm diode lasers in oral facial practice: current state of the science and art. Int J Med Sci. 2009; 6: 358-364.
- Yagüe-García J, España-Tost AJ, Berini-Aytés L, Gay-Escoda C. Treatment of oral mucocele-scalpel versus C02 laser. Med Oral Patol Oral Cir Bucal. 2009; 14: e469-74.
- Strauss RA, Jones G, Wojtkowski DE. A comparison of postoperative pain parameters between CO2 laser and scalpel biopsies. J Oral Laser Appl. 2006; 6: 39-42.