
Open Journal of
Clinical and Medical Images
Clinical Image - Open Access, Volume 3
Body stalk anomaly
*Corresponding Author: Kentaro Okamoto
Department of Pediatric Surgery, Tokyo Medical and Dental University, Yushima 1-5-45, Bunkyo-ku, Tokyo,113-8519, Japan.
Tel: +81-03-5803-5261 & +81-03-5803-0138;
Email: okasrg2@tmd.ac.jp
Received : Jul 31, 2023
Accepted : Aug 23, 2023
Published : Aug 31, 2023
Archived : www.jclinmedimages.org
Copyright : © Okamoto K (2023).
Citation: Okamoto K. Body stalk anomaly. Open J Clin Med Images. 2023; 3(2): 1133.
Clinical image description
A 29-year-old pregnant woman was referred to our hospital at the gestational age of 15 weeks. The umbilical cord hernia was pointed out during a fetal echocardiogram at the previous obstetrician’s office, and the patient was referred to our obstetrician. An MRI scan of the fetus was performed at 30 weeks and 3 days after conception, and showed intra-abdominal organ prolapse, right kidney defect, right lower limb defect, and flexion deformity of the spinal column (Figure 1). At 34 weeks 6 days of gestation, her water broke, and she was born by emergency cesarean section. She weighed 1262 g and had an Apgar score of 3/4. Postnatal physical examination revealed prolapse of intra-abdominal organs (liver, stomach, entire intestinal tract, and bladder) (Figure 2). The perineum was also dysplastic, and a cloaca was present; a diagnosis of body stalk anomaly was made, and the prolapsed organs were covered with sterile plastic at day 0. An enterostomy was created at day 1, and the prolapsed organ was covered with a hernia sac to await epithelialization (Figure 3). The prolapsed organ was epithelialized, dried, and settled down, but at age 69, the patient developed respiratory failure due to pulmonary congestion and died permanently (Figure 4).
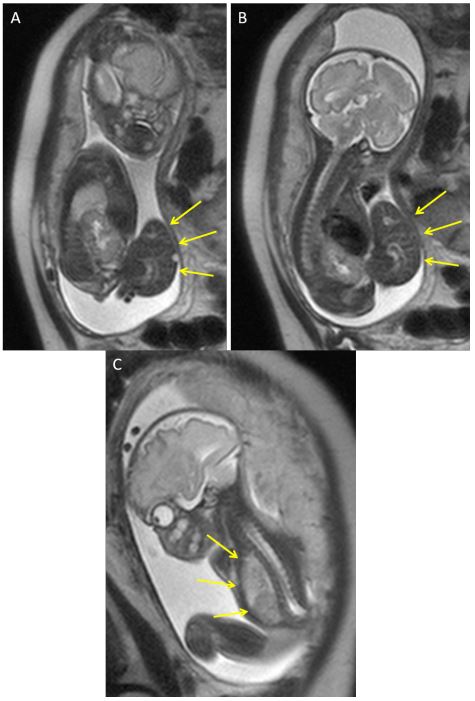
A,B: There was a giant omphalocere. Digestive tracts was out of abdominal wall.
C: Lung was hyperinflation.

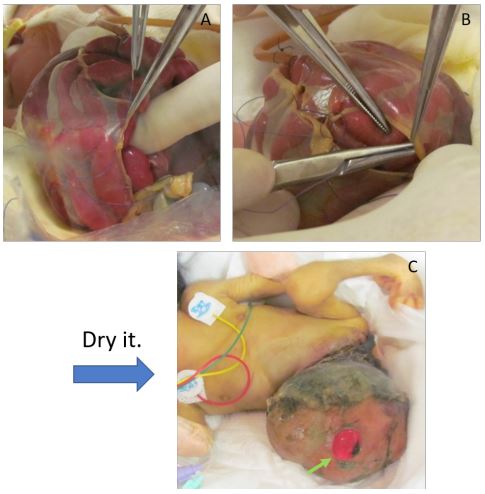
A,B: Prolapsed organs were covered with hernial sac at day 1.
C: The hernia sacs were dried. The perforated area was used as an enterostomy (arrow).

Kermauner first described BSA, in 1906, as an abdominal wall defect consisting of an amniotic sac, which contains viscera and is directly attached to the placenta, in the absence of an umbilical cord [1]. Van Allen et al. set forth the diagnostic criteria for BSA in 1987. Two of the following three anomalies must be present to establish a positive diagnosis [2,3].
Exencephaly/encephalocele with facial clefts.
Thoracoschisis and abdominoschisis (midline defect).
Limb defect (for example, clubfoot, polydactyly, oligodactyly, syndactyly, brachydactyly, amelia).
Declarations
Acknowledgement: None.
Conflict of interest: No conflict of interest
Consent: Written informed consent has been obtained from the mother of patient.
References
- Kermauner F. Die Missbildungen des Rumpfes. In: Schwalbe E, Gruben GB (eds). Die Morfologie der Miβbildungen des Menschen and der Tiere. 3rd edition, Gustav Fischer Verlag, Jena, Germany. 1906; 41-85.
- Van Allen M, Curry C, Gallagher L. Limb-body wall complex: I. Pathogenesis. Am J Med Genet. 1987; 28: 529-548.
- Kocherla K, Kumari V, Kocherla PR. Prenatal diagnosis of body stalk complex: A rare entity and review of literature. Indian J Radiol Imaging. 2015; 25: 67-70.