
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 3
Hemorrhagic cholecystitis causing an intrahepatic subcapsular hematoma: Case report and review of the literature
Y Sur*; A Atay; ON Dilek
Departmantl of General Surgery, Izmir Katip Celebi University Atatürk Education and Research Hospital, Izmir, Turkey.
*Corresponding Author: Yunus Sur
Atatürk Training and Research Hospital Press Site -
Izmir 35360/Turkey.
Tel: +90-0232-244-44-44;
Email: dr.yunus.sur@gmail.com
Received : Aug 28, 2023
Accepted : Sep 20, 2023
Published : Sep 27, 2023
Archived : www.jclinmedimages.org
Copyright : © Sur Y (2023).
Abstract
Hemorrhagic cholecystitis is a very rare condition. It can present very different clinical symptoms. It often occurs as a complication of cholecystitis. These patients are usually under anticoagulant therapy or they have coagulopathy. Patients present to the hospital with a wide variety of clinical situations such as cholestasis, hemorrhagic shock, acute abdomen.
Intrahepatic subcapsular hematoma is also very rare. It occurs secondary to trauma or invasive procedures, and as in our case, it may also occur due to hemorrhagic cholecystitis. It can be a life-threatening condition.
In both clinical situations, various treatment options are available. We must prefer the appropriate treatment method such as surgery, percutaneous intervention, selective embolization, and medical follow-up according to each patient.
In this case, we aimed to present a case of an intrahepatic subcapsular hematoma due to hemorrhagic cholecystitis under anticoagulant treatment in the light of literature data.
As far as we know, our case is the first case of hemorrhagic cholecystitis in the literature that causes an intrahepatic subcapsular hematoma.
Keywords: Gallbladder; Hemorrhage; Hematoma.
Citation: Sur Y, Atay A, Dilek ON. Hemorrhagic cholecystitis causing an intrahepatic subcapsular hematoma: Case report and review of the literature. Open J Clin Med Images. 2023; 3(2): 1139.
Introduction
Hemorrhagic cholecystitis is a rare condition that presents with different symptoms. It usually occurs as a complication of acute cholecystitis. It may also occur due to malignancy, trauma, bleeding diathesis, cirrhosis, percutaneous interventions, renal failure, and anticoagulant use [1].
Cases of intrahepatic subcapsular hematoma are very rare. It usually occurs after a trauma or interventional procedures. It has high mortality and morbidity rates like hemorrhagic cholecystitis. So, follow-up and treatment are difficult [2].
In this article, we aimed to present our case of intrahepatic subcapsular hematoma due to hemorrhagic cholecystitis in light of literature data.
Case
An 82-years-old male patient admitted to emergency service with right upper abdominal pain for 5 days and high fever (39.2°C) for 2 days. He had a history of acute cholecystitis. He was using an anticoagulant (edoxaban) due to heart failure and atrial fibrillation.
On physical examination, the patient had tenderness and palpable stiffness in the right upper quadrant. There was no involuntary defense and rebound. On admission lab tests, white blood cell: 32.42×103/ml3 , hemoglobin: 10.4 g/dl, platelet count: 459.000/ml3 , total bilirubin: 2.1 mg/dl, AST: 186 Iu/l, ALT: 194 Iu/l, INR: 2, kreatin: 2.56.
Ultrasonography (USG) findings of the patient: The gallbladder had a hydropic appearance, wall thickness had increased. Also, there were stones and an image of high echogenicity in the gallbladder. This view was consistent with hemorrhagic cholecystitis. On the surface of the right lobe of the liver, there was a heterogeneous collection.
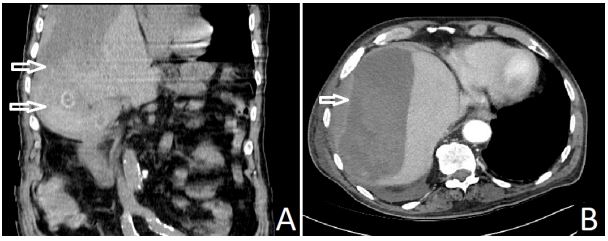
Abdominal Computed Tomography (CT) findings of the patient were similar to USG findings (Figure 1). In CT, there wasn’t active arterial bleeding in the gallbladder. Also, the superior of the fundus of the gallbladder was curve and joined to the liver capsule. We saw a collection of 15x9 cm with clear borders starting from here. This was consistent with an intrahepatic subcapsular hematoma. The patient had no history of trauma or surgical procedures. So, we detected the perforation of the hemorrhagic cholecystitis content into the subcapsular region of the right lobe of the liver.
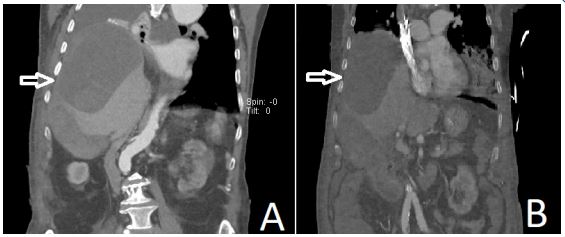
In the radiological follow-up, there wasn’t an increase in the size of the intrahepatic subcapsular hematoma of the patient. We didn’t see free fluid in the abdomen. In laboratory tests, the hemoglobin amount of the patient did not decrease. We decided on medical follow-up due to the patient’s stable hemodynamics and the presence of many comorbid diseases. On the 5th day of follow-up, atrial fibrillation with rapid ventricular response and pleural effusion occurred. On the 7th day of followup, we intubated and transferred the patient to the intensive care unit. During the follow-up of the patient, we scanned 3 CT and 3 USG images. We didn’t see an increase in hematoma size in any of them (Figure 2). Despite all efforts, we could not cure the patient’s respiratory problems. The patient died in intensive care on the 23rd day of follow-up.
Discussion
Hemorrhagic cholecystitis occurs due to a transmural inflammation that leads to ischemia and mucosal deterioration in the gallbladder wall. It causes erosion in the gallbladder vessels. It then causes bleeding into the gallbladder lumen or the abdominal cavity [3].
The hemorrhagic cholecystitis clinic can mimic many clinical conditions, from cholestasis to hemorrhagic shock. In hemorrhagic cholecystitis, If a blood clot obstructs the biliary ducts, obstructive jaundice may occur in the patient. If the gallbladder ruptures, bleeding can occur into the abdominal cavity. In this case, the clinical picture can progress to hemorrhagic shock. In the patient we presented, hemorrhagic cholecystitis has ruptured into the intrahepatic subcapsular area. Therefore, the bleeding in the patient accumulated in this cavity, and the hematoma was formed. So, signs of generalized peritonitis and hemorrhagic shock hasn’t occurred in the patient.
Hemorrhagic cholecystitis may present as a complication of anticoagulation therapy. It's a rare but fatal complication [4]. We should be careful especially in patients using anticoagulants. Also our case, there was a 5-year history of edoxaban use. With the launch of a new generation of oral anticoagulants, the incidence of hemorrhagic cholecystitis may increase [4]. With the widespread use of such drugs, the management of emergency surgical procedures in patients using these drugs has become more complex.
In hemorrhagic cholecystitis, imaging methods are more helpful in diagnosis than examination and laboratory findings. We see intraluminal membranes and echogenic material and thickening of the gallbladder wall on USG. But we may encounter similar images in other gallbladder diseases. In this case, scanning the abdomen with CT and showing active arterial bleeding in the gallbladder may be more specific for diagnosis [1,4].
There are cases of intrahepatic subcapsular hematoma reported after laparoscopic cholecystectomy, ERCP, and percutaneous cholecystostomy. But, the pathophysiology of intrahepatic subcapsular hematoma has not been completely elucidated. It has been suggested that traction during surgical or interventional procedures and using guide wires may damage the liver capsule and parenchymal vessels or may be due to bleeding from existing hemangiomas [2,5]. In our case, there was no history of recent trauma or interventional procedure. So, we deduce that intrahepatic hematoma was secondary to existing hemorrhagic cholecystitis.
In intrahepatic subcapsular hematoma, signs of liver failure may occur in the patient. On imaging, we can see ischemic liver parenchyma, narrowing of hepatic veins due to hematoma. In this case, we should be careful about hepatic compartment syndrome. In these patients, percutaneous drainage of the hematoma can be life-saving.
Treatment of hemorrhagic cholecystitis is usually cholecystectomy. We may use cholecystostomy in selected patients. There are various treatment options for intrahepatic subcapsular hematoma. These are conservative follow-up, percutaneous drainage, selective embolization, and surgical interventions. In the case of hemorrhagic cholecystitis with intrahepatic subcapsular hematoma, if surgical treatment is a high risk if there isn't an increase in hematoma size, and there isn't hepatic compartment syndrome in hemodynamically stable patients, conservative treatment is appropriate [2,3,5].
Conclusion
In conclusion, We should not forget that hemorrhagic cholecystitis can have fatal complications such as intrahepatic subcapsular hematoma in patients under anticoagulant therapy. In these patients, conservative treatment may be possible with close follow-up with USG and CT.
Declarations
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Sweeny A, Smith NA, Serfin JA. Hemorrhagic cholecystitis causing hemobilia and common bile duct obstruction. J Surg Case Rep. 2019; 2019: rjz081.
- Minaya Bravo AM, González González E, Ortíz Aguilar M, Larrañaga Barrera E. Two rare cases of intrahepatic subcapsular hematoma after laparoscopic cholecystectomy. Indian J Surg. 2010; 72: 481-484.
- Morris DS, Porterfield JR, Sawyer MD. Hemorrhagic cholecystitis in an elderly patient taking aspirin and cilostazol. Case Rep Gastroenterol. 2008; 2: 203-207.
- Kinnear N, Hennessey DB, Thomas R. Haemorrhagic cholecystitis in a newly anticoagulated patient. BMJ Case Rep. 2017; 2017: bcr2016214617.
- Zappa MA, Aiolfi A, Antonini I, Musolino CD, Porta A. Subcapsular hepatic haematoma of the right lobe following endoscopic retrograde cholangiopancreatography: Case report and literature review. World J Gastroenterol. 2016; 22: 4411-4415.