
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 3
Choroidal detachment associated with orbital cellulitis: A rare clinical finding
Zoe N Anderson, BS1*; Kayla A Aikins, BS1; Ryan Nolan, BS1; Nicholas Matthees, MD2
1University of Nevada, Reno School of Medicine, Reno, NV, USA.
2Department of Neuroradiology, Barrow Neurological Institute, Phoenix, AZ, USA.
*Corresponding Author: Zoe Anderson
University of Nevada, Reno School of Medicine,
1664 N. Virginia St., Reno, NV 89557, USA.
Email: zoeanderons@med.unr.edu
Received : Nov 23, 2023
Accepted : Dec 20, 2023
Published : Dec 28, 2023
Archived : www.jclinmedimages.org
Copyright : © Anderson Z (2023).
Abstract
Orbital cellulitis is an infection involving the ocular adnexal structures posterior to the orbital septum, and can develop secondary to sinus infection, trauma to the eye, local infection of the mouth or face, or spread of periorbital cellulitis. Classic symptoms include swelling, redness, fever, tenderness, pain with eyeball movement, double vision, blurry vision, and proptosis. Rarely, choroidal detachment, occurring when fluid accumulates between the choroid and the sclera, can occur as a manifestation of orbital cellulitis. We present a case of orbital cellulitis with choroidal detachments, suspected to be secondary to orbital cellulitis, and describe the corresponding CT and MRI findings.
Keywords: Orbital cellulitis; choroidal detachments; Orbital cellulitis concurrent choroidal detachments; CT orbital cellulitis; CT choroidal detachments.
Citation: Anderson Z, Aikins KA, Nolan R, Matthees N. Choroidal detachment associated with orbital cellulitis: A rare clinical finding. Open J Clin Med Images. 2023; 3(2): 1159.
Introduction
Orbital cellulitis is an infective process that involves the ocular adnexal structures posterior to the orbital septum [1]. Orbital cellulitis can result as a complication of sinus infection, trauma to the eye, infection of the tear duct, teeth, or face, or spread of periorbital cellulitis [2]. Symptoms can include periorbital swelling, redness, fever, tenderness, pain with eyeball movement, double vision, blurry vision, and proptosis [3]. Orbital cellulitis can result in local abscess or intracranial abscess, vision loss, or even death [2]. Treatment requires IV antibiotics and may require surgical management. Choroidal detachment, a condition in which fluid accumulates within the suprachoroidal space, is a rare and severe manifestation of orbital cellulitis [4,5].
Case presentation
A 71-year-old woman with a history of recent stroke, cataracts, and type II diabetes presented to the emergency department with worsening right eye swelling and redness. Reports from the patient’s team reported initial symptoms of “pink eye” related to a suspected corneal ulcer. The patient had seen an optometrist in the outpatient setting regarding these symptoms. The patient was started on topical antibiotics in the outpatient setting. However, she presented to the emergency department with worsening redness and pain a few days after topical treatment initiation.
Tense, diffuse, erythematous lid swelling, substantial rightsided proptosis with a tense globe and reduced ballotment, and pain with eye movements were appreciated on physical exam. Given that physical exam findings were concerning for orbital cellulitis, CT was indicated and performed. Orbital cellulitis was confirmed in addition to the finding of choroidal detachment. Two days later, an MRI was obtained for further evaluation to ensure no abscess formed.
The patient was started on IV vancomycin and cefepime, as well as topical tobramycin and trimethoprim/polymyxin B and monitored for signs of encephalitis. Cultures grew Pseudomonas aeruginosa and Staphylococcus aureus.
Discussion
Orbital cellulitis is an inflammatory process of the muscles and fat posterior to the orbital septum [6]. Orbital cellulitis can occur in any age group, but more commonly occurs in pediatric patients [7]. The infectious agent is typically bacterial and can be polymicrobial, including fungal organisms or mycobacteria [7]. Choroidal detachment, a rare manifestation of orbital cellulitis, occurs when fluid accumulates between the choroid and the sclera [5]. Choroidal detachments are most commonly attributed to eye surgery, trauma, cancer, and medications rather than orbital cellulitis [8]. Choroidal detachment risk factors include: recent eye surgery, blood thinner usage, nanophthalmos, eye trauma, eye inflammation, advanced age, atherosclerosis, glaucoma, and history of choroidal detachment in the contralateral eye [9].
Because of its rarity, differential diagnoses for choroidal detachment should be considered. One such differential is preseptal cellulitis, an infection affecting the soft tissue of structures anterior to the orbital septum, including the eyelid and skin around the eye [3]. By definition, there is no orbital involvement, and it is less likely to lead to severe complications [3]. It is necessary to differentiate preseptal cellulitis from orbital cellulitis, as preseptal cellulitis can be treated in the outpatient setting with oral antibiotics, unlike orbital cellulitis, which must be treated with IV antibiotics [2]. Differentiating factors include that preseptal cellulitis usually does not alter vision or cause painful eye movements, while orbital cellulitis can cause blurry vision, diplopia, proptosis, and painful eye movements [2]. Another differential diagnosis includes orbital pseudotumor, which presents as a palpable mass and swollen eyelid, at times bilateral [10]. Patients often exhibit diminished ocular motility, sometimes with decreased visual acuity. A biopsy may be necessary to confirm diagnosis [10]. We report an atypical manifestation of orbital cellulitis with choroidal detachment, assumed to be secondary to infection. This condition is a medical emergency requiring prompt treatment to prevent blindness, meningitis, or death [11]. Imaging is indicated in suspected cases to distinguish orbital cellulitis from the less severe and more common preseptal cellulitis.
Associations of choroidal detachments include serous retinal detachment, secondary angle closure glaucoma, and a very shallow anterior chamber [5]. Sequelae of choroidal detachment include decreased visual acuity, ocular pain, vomiting, nausea, and loss of vision [5]. Orbital cellulitis requires IV antibiotics and may require surgery [3]. A previously described case of choroidal detachment likely secondary to orbital cellulitis also included steroid administration to address the chemosis, as well as anticoagulant use to prevent cavernous sinus thrombosis [4]. Medical therapies to treat choroidal detachment may consist of topical cycloplegia and corticosteroids topically and/ or orally [5].

Conclusion
This report documents the manifestation of orbital cellulitis accompanied by choroidal detachment, suggesting a plausible infectious origin. Orbital cellulitis, an inflammatory process affecting the muscles and adipose tissue situated posterior to the orbital septum, emerges as a critical medical concern demanding immediate intervention to avert potential outcomes of blindness, meningitis, or even mortality [7]. Employing imaging techniques becomes imperative in suspected cases to differentiate orbital cellulitis from the more prevalent and less severe preseptal cellulitis. Choroidal detachments, an infrequent occurrence, consist of the accumulation of fluid between the choroid and the sclera [4]. While these detachments are more commonly associated with factors like ocular surgery, trauma, neoplasms, and medications (albeit even rare in such contexts), their connection to orbital cellulitis remains remarkably atypical [5]. Associations encompass serous retinal detachment, secondary angle closure glaucoma, and an unusually shallow anterior chamber [5]. This uncommon scenario involving orbital cellulitis featuring choroidal detachment, potentially rooted in infection, underscores the value of CT and MRI and the vital role of the radiologist in making a rapid diagnosis.
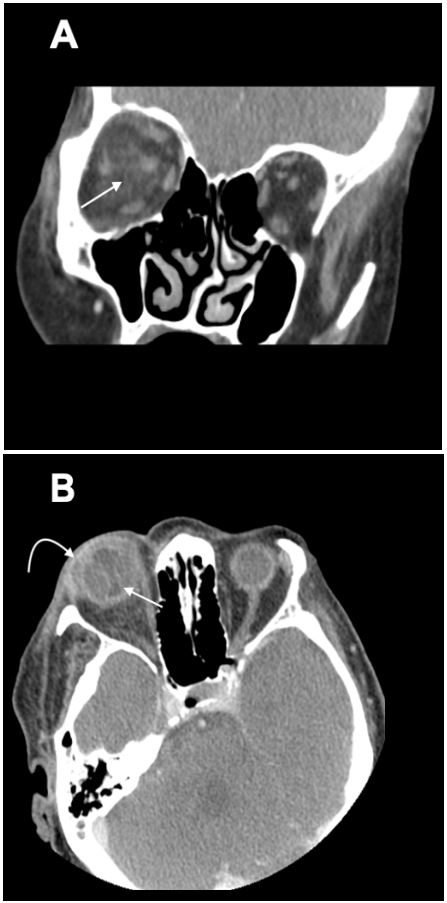
Images: MRI of orbital cellulitis shows inflammation and swelling of the extraocular muscles and intraconal fat. Soft-tissue thickening and proptosis may also be present. In this case, choroidal detachment accompanies orbital cellulitis and appears as a thickened line of increased density within the vitreous with a characteristic “hourglass” shape. Inflammation produces accumulation of position-dependent fluid.
References
- Connell B, Kamal Z, McNab AA. Fulminant orbital cellulitis with complete loss of vision. Clin Exp Ophthalmol 2001; 29: 260-261.
- Baiu I, Melendez E. Periorbital and Orbital Cellulitis. JAMA. 2020; 323(2): 196. doi:10.1001/jama.2019.18211.
- Milo R. Preseptal Cellulitis Versus Orbital Cellulitis. Advanced Emergency Nursing Journal. 2022; 44(3):199-205. doi: 10.1097/TME.0000000000000416.
- Farhi P, Kurup S. & Abdelghani W. Orbital cellulitis associated with combined retinal and choroidal detachments. 2007; 1009-1010https://doi.org/10.1038/sj.eye.6702815.
- Diep MQ, Madigan MC. Choroidal detachments: what do optometrists need to know? Clin Exp Optom. 2019; 102(2): 116-125. doi: 10.1111/cxo.12807. Epub 2018 Jul 4. PMID: 29971817.
- Tsirouki T, Dastiridou AI, Ibánez Flores N, Cerpa JC, Moschos MM, Brazitikos P, Androudi S. Orbital cellulitis. Surv Ophthalmol. 2018; 63(4): 534-553. doi: 10.1016/j.survophthal.2017.12.001. Epub 2017 Dec 15. PMID: 29248536.
- Danishyar A, Sergent SR. Orbital Cellulitis. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2022. https://www.ncbi.nlm.nih.gov/books/NBK507901/: https://www.ncbi.nlm.nih.gov/books/NBK507901/#:~:text=Although%20orbital%20cellulitis%20can%20occur,and%20even%20fungal%20or%20mycobacteria.
- Fujikawa A, Kitaoka T, Miyamura N, Amemiya T. Choroidal detachment after vitreous surgery. Ophthalmic Surg Lasers. 2000; 31(4): 276-81. PMID: 10928663.
- The American Society of Retina Specialists. Choroidal Detachment. Choroidal Detachment - Patients - The American Society of Retina Specialists. 2023. https://www.asrs.org/patients/retinal-diseases/11/choroidal-detachment.
- Mendenhall WM, Lessner AM. Orbital pseudotumor. Am J Clin Oncol. 2010; 33(3): 304-6. doi: 10.1097/COC.0b013e3181a07567.PMID: 19738455.
- Kyari F. Emergency management: orbital cellulitis. Community Eye Health. 2018; 31(103): 60. PMID: 30487680; PMCID: PMC6253316.