
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
First report of an appendiceal perforation caused by a migrated biliary stent after orthotopic liver transplantation
Ferraro D1*; Maniscalco M1; Arenga G1; Falaschi F1; Galeota Lanza A2; Vennarecci G1
1UOC Hepato-Biliary Surgery and Liver Transplant Centre, AORN Antonio Cardarelli, Naples, Italy.
2UOC Hepatology, AORN Antonio Cardarelli, Naples, Italy.
*Corresponding Author: Daniele Ferraro
UOC Hepatobiliary Surgery and Liver Transplant Centre,
AORN Antonio Cardarelli, Naples, Italy.
Email: daniele.ferraro@aocardarelli.it
Received : Dec 05, 2023
Accepted : Jan 10, 2024
Published : Jan 17, 2024
Archived : www.jclinmedimages.org
Copyright : © Ferraro D (2024).
Abstract
Keywords: Liver transplantation; Biliary stent; Liver cirrhosis; Appendiceal perforation.
Citation: Ferraro D, Maniscalco M, Arenga G, Falaschi F, Galeota Lanza A, et al. First report of an appendiceal perforation caused by a migrated biliary stent after orthotopic liver transplantation. Open J Clin Med Images. 2024; 4(1): 1161.
Introduction
The overall incidence of biliary strictures in liver transplanted patients is around 13% [1], mostly located at the biliary anastomosis, occurring from 6 to 12% of cases [2]. The first treatment option of anastomotic biliary strictures is the insertion of a plastic or metallic biliary prosthesis with endoscopic retrograde cholangiopancreatography (ERCP). Distal migration of biliary stent is an unusual complication related to this procedure, occurring in about 6% of patients [3], but in literature cases of abdominal visceral perforation due to this complication are described, mainly involving small intestine and colon [4-6]. An isolated case of appendiceal perforation related to stent dislocation is found in literature [6].
Case report
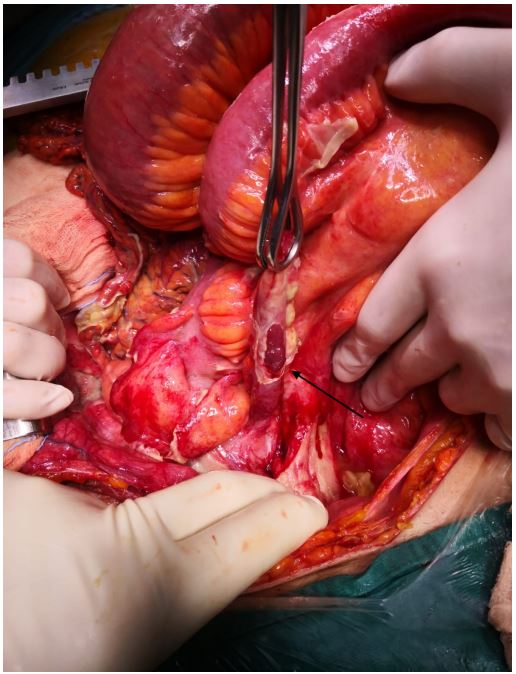
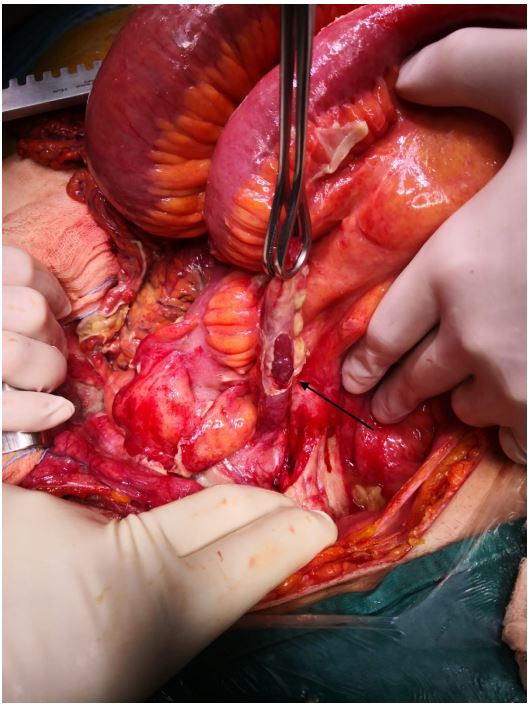
A 63-year-old male patient with a history of orthotopic liver transplantation in June 2021 underwent an ERCP procedure in October 2021 for the treatment of anastomotic biliary stricture. Three months later, he came to the emergency department for acute onset abdominal pain and localized peritonitis in the right lower quadrant, emesis, anorexia, and acute kidney failure. Blood tests showed neutrophile leukocytosis, elevated C-reactive protein (400 mg/ml) and preserved liver function. A plain abdominal X-ray detected a foreign body in the right iliac fossa, more likely the dislocated biliary prosthesis. An abdominal CT scan with contrast enhancement confirmed the dislocation of the biliary prosthesis in the right iliac fossa and the presence of free abdominal air and multiple fluid-filled collection [Figure 1]. Suspicion of cecal or appendiceal perforation was posed. Therefore, the patient underwent an urgent exploratory laparotomy that showed appendiceal perforation caused by the dislocated biliary stent (Figures 2 and 3); the stent was extracted, appendicectomy performed and the peritoneal cavity washed to evacuate the abscesses. Post-operative course was featured with ileus and the need of a second-look laparotomy for wash out of residual fluid collection. Two years after surgery the patient is alive and fully recovered.

Discussion
Dislocation of biliary stent is an uncommon complication related to ERCP with an incidence of 3-6%. It can migrate proximally or distally in the biliary duct. Distal migration is more likely in case of benign disease, papillary stenosis, use of straight stents (compared to pigtail), sphincterotomy, common bile duct diameter >10 mm and use of larger stents [7]. In 43% of cases, migrated biliary prosthesis are spontaneously eliminated with evacuation [8]. When endoscopic access is available, endoscopic treatment of migrated biliary stent becomes the first choice [9,10]. Intestinal perforation is a rare consequence of biliary prosthesis distal migration [11]. Extrinsic fixation of the bowel secondary to postoperative bowel adhesion, diverticulosis, hernia, or stricture is a risk factor for stuck biliary stent in the intestinal wall, increasing the chance of visceral perforation [12,13]. Intestinal perforation requires prompt investigation and urgent surgical treatment for stent removal and drainage of intra-peritoneal or retroperitoneal abscesses [14]. Duodenum is the most frequent site of perforation reported in literature [15]. Perforations in the liver, sigmoid colon, caecum, and pancreas are also described in different studies [4,16]. As far as we are concerned, only one case report of an appendiceal perforation occurred after ERCP in a patient affected by chemotherapy-induced neutropenic enterocolitis is described in literature. A conservative treatment with broad-spectrum antibiotics, fluid resuscitation, correction of hematological parameters was the first choice due to the high surgical and anesthesiologic risk of the patient; after an unsuccessful endoscopic attempt, it was surgically removed and appendicectomy was performed with local lavage and drain placement [6]. So far, in English literature, there is no report of appendiceal perforation due to biliary stent migration in a liver transplant recipient. We believe that in the setting of iatrogenic immunosuppression after liver transplantation, the possible consequences of appendiceal perforation could be catastrophic and the management of these patients require high suspicion index to diagnose the condition, prompt definition of therapeutic plan and fine post-operative management, including modulation of immunosuppression in order to balance the risk of overwhelming sepsis and rejection, especially if the perforation occurs in the very first months after transplantation.
References
- Akamatsu N, Sugawara Y, Hashimoto D. Biliary reconstruction, its complications and management of biliary complications after adult liver transplantation: a systematic review of the incidence, risk factors and outcome. Transpl Int 2011; 24: 379-392.
- Sharma S, Gurakar A, Jabbour N. Biliary strictures following liver transplantation past, present and preventive strategies. Liver Transpl 2008; 14: 759-769.
- Namdar T, Raffel AM, Topp SA, Namdar L, Alldinger I, Schmitt M, Knoefel WT, Eisenberger CF. Complications and treatment of migrated biliary endoprostheses: a review of the literature. World J Gastroenterol. 2007; 13(40): 5397-9. doi: 10.3748/wjg.v13.i40.5397. PMID: 17879415; PMCID: PMC4171335.
- Park TY, Hong SW, Oh HC, Do JH. Colonic diverticular perforation by a migrated biliary stent: A case report with literature review. Medicine (Baltimore). 2021; 100(52): 28392. doi: 10.1097/MD.0000000000028392. PMID: 34967373; PMCID: PMC8718208.
- Esterl RM Jr, St Laurent M, Bay MK, Speeg KV, Halff GA. Endoscopic biliary stent migration with small bowel perforation in a liver transplant recipient. J Clin Gastroenterol. 1997; 24(2): 106-10. doi: 10.1097/00004836-199703000-00014. PMID: 9077729.
- Pengermä P, Katunin J, Turunen A, Sileri P, Giarratano G, Palomäki A, Kechagias A. Appendiceal perforation due to biliary stent migration in a neutropenic patient with lung cancer receiving chemotherapy: A case report. Mol Clin Oncol. 2021; 15(1): 136. doi: 10.3892/mco.2021.2298. Epub 2021 May 17. PMID: 34055351; PMCID: PMC8145604.
- Johanson JF, Schmalz MJ, Geenen JE. Incidence and risk factors for biliary and pancreatic stent migration. Gastrointest Endosc. 1992; 38(3): 341-346. doi: 10.1016/S0016-5107(92)70429-5.
- Cerisoli C, Diez J, Giménez M, Oria M, Pardo R, Pujato M. Implantation of migrated biliary stents in the digestive tract. HPB (Oxford). 2003; 5(3): 180-2. doi: 10.1080/13651820310015301. PMID: 18332981; PMCID: PMC2020584.
- Gromski MA, Bick BL, Vega D, Easler JJ, Watkins JL, Sherman S, Lehman GA, Fogel EL. A rare complication of ERCP: duodenal perforation due to biliary stent migration. Endosc Int Open. 2020; 8(11): E1530-E1536. doi: 10.1055/a-1231-4758. Epub 2020 Oct 21. PMID: 33140007; PMCID: PMC7577786.
- Matsumoto K, Katanuma A, Maguchi H. Endoscopic removal technique of migrated pancreatic plastic stents. J Hepatobiliary Pancreat Sci. 2014; 21(6): E34-40. doi: 10.1002/jhbp.94. Epub 2014 Feb 17. PMID: 24535753.
- Størkson RH, Edwin B, Reiertsen O, Faerden AE, Sortland O, Rosseland AR. Gut perforation caused by biliary endoprosthesis. Endoscopy. 2000; 32(1): 87-9. doi: 10.1055/s-2000-87. PMID: 10691280.
- Mistry BM, Memon MA, Silverman R, Burton FR, Vanna CR, Solomon H, Garvin PJ Small bowel perforation from a migrated biliary stent. Surg Endosc .2001; 15: 1043.
- Wilhelm A, Langer C, Zoeller G, et al. Complex colovesicular fistula: a severe complication caused by biliary stent migration. Gastrointest Endosc 2003; 57: 124-6.
- Diller R, Senninger N, Kautz G, Tübergen D. Stent migration necessitating surgical intervention. Surg Endosc. 2003; 17(11): 1803-7. doi: 10.1007/s00464-002-9163-5. Epub 2003 Sep 29. PMID: 14508668.
- Stassen PMC, de Jong DM, Poley JW, Bruno MJ, de Jonge PJF. Prevalence of and risk factors for stent migration-induced duodenal perforation. Endosc Int Open. 2021; 9(3): 461-469. doi: 10.1055/a-1337-2321. Epub 2021 Feb 19. PMID: 33655050; PMCID: PMC7895667.
- Barut I, Tarhan OR. Cecum perforation due to biliary stent migration. Saudi Med J. 2014; 35(7): 747-49