
Open Journal of
Clinical and Medical Images
Case Series - Open Access, Volume 4
Fibro-adipose vascular anomaly: A clinico-radiologic review
Nikshita Jain1; Madhavi Kandagaddala1; Emil Genistopher2; Jonathan Reddy2; Arun Hulsoore2; Thomas Palocaren2*
1Department of Radiology, Christian Medical College, Vellore, Tamil Nadu, India.
2Department of Pediatric Orthopedics, Christian Medical College, Vellore, Tamil Nadu, India.
*Corresponding Author: Thomas Palocaren
Department of Pediatric Orthopedics Christian Medical
College, Vellore, Tamil Nadu, India.
Email: thomaspalox@cmcvellore.ac.in
Received : Dec 21, 2023
Accepted : Jan 16, 2024
Published : Jan 23, 2024
Archived : www.jclinmedimages.org
Copyright : © Palocaren T (2024).
Abstract
Fibro-adipose vascular anomaly remains in the ‘provisionally unclassified’ group of the ISSVA classification of vascular anomalies, since being first described in 2014. We present a series of 22 children diagnosed as FAVA, describing the presentation, findings on imaging and treatment strategies at a tertiary care hospital in southern India.
Keywords: FAVA; Rare Vascular Anomalies; Pediatric vascular anomalies.
Abbreviations: FAVA: Fibroadipose vascular anomaly; ISSVA: International Society for the Study of Vascular Anomalies; VM: venous malformation; MRI: Magnetic resonance imaging.
Citation: Jain N, Kandagaddala M, Genistopher E, Reddy J, Palocaren T, et al. Fibro-adipose vascular anomaly: A clinicoradiologic review. Open J Clin Med Images. 2024; 4(1): 1163.
Introduction
Since its first description in 2014 by Alomari et al at Boston Children’s Hospital [1], FAVA remains in the provisionally unclassified group in the ISSVA classification. While it has unique clinical, radiological and histopathological features that allow for its diagnosis [1], the management strategy and techniques are still evolving with no consensus yet regarding a standardised approach. Over 22 children presented to our institute with extremity pain and swelling, and proven to have FAVA by imaging and histopathology, in the last 10 years. We will illustrate 3 children with histopathologically proven FAVA in different locations.
Case review
Of a total 22 children, 14 were in the 10-12 age group and unlike most recent studies [1,4,5], the proportion of boys was marginally higher than girls (13:10). All the children presented with extremity pain and swelling, with contractures seen in 3 out of 22 children. 4 children had an antecedent history of trivial trauma to the site, prior to onset of pain. While 12 children had lesions involving either the gastrocnemius or soleus (10 involving gastrocnemius and 2 soleus), the remaining 11 children had varying sites of muscle involvement, namely the thigh, gluteal region and foot. None had upper extremity involvement. 10 children had a direct surgical excision, while 8 underwent sclerotherapy. 1 child had both excision with sclerotherapy for recurrence, and 2 of the children also had contracture release surgeries. Three of our patients are being managed conservatively.
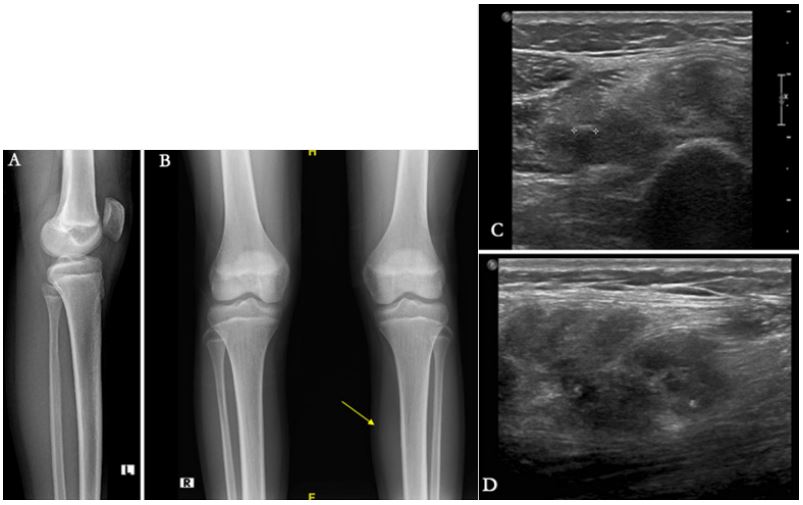
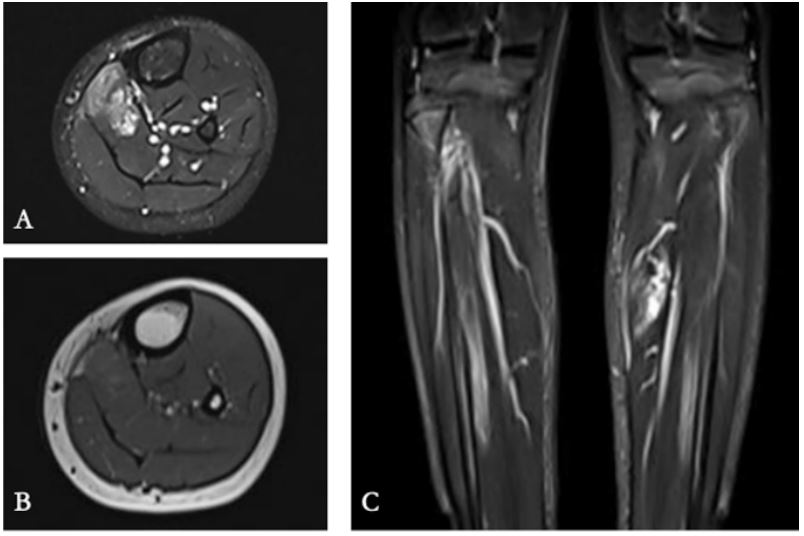
Case 1: A 12 year old boy presenting with calf pain and swelling of 2 years duration. Antecedent history of blunt trauma to the site was present, following fall from bike, prior to onset of pain. No history of fever present. On clinical examination, a diffuse soft tissue swelling was noted over the upper one-third of the posteromedial aspect of the leg. There was no restriction of movement. As depicted in Figure 1, no significant bony changes were seen on the radiograph, while ultrasound revealed an intramuscular soft tissue lesion showing calcification within. MRI (Figure 2) further illustrates the fatty component within the lesion, seen as hyperintensity on T1 weighted images, with an otherwise heterogenously hyperintense appearance on T2 weighted images. Complete surgical excision was carried out and histopathology revealed features typical for FAVA, namely lymphoid aggregates and entrapped nerve fibres were seen.
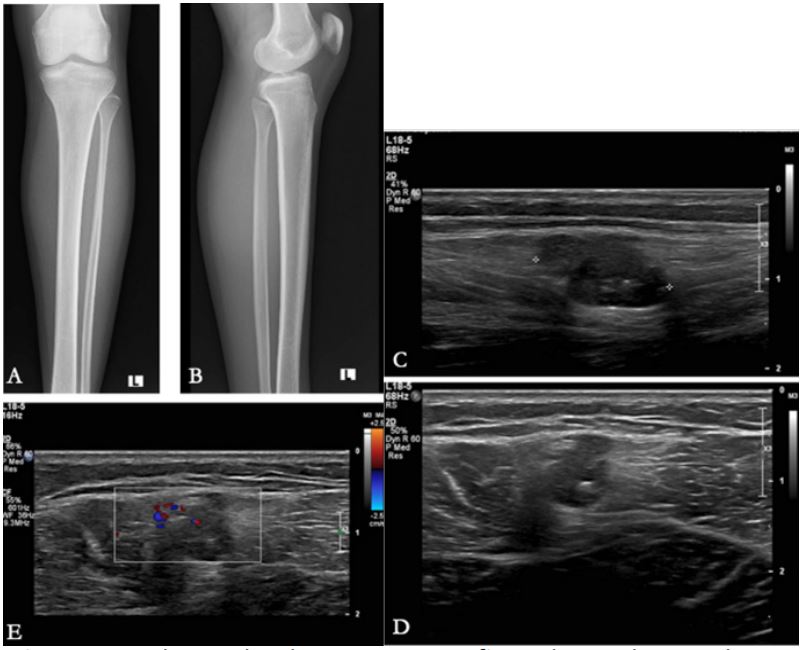
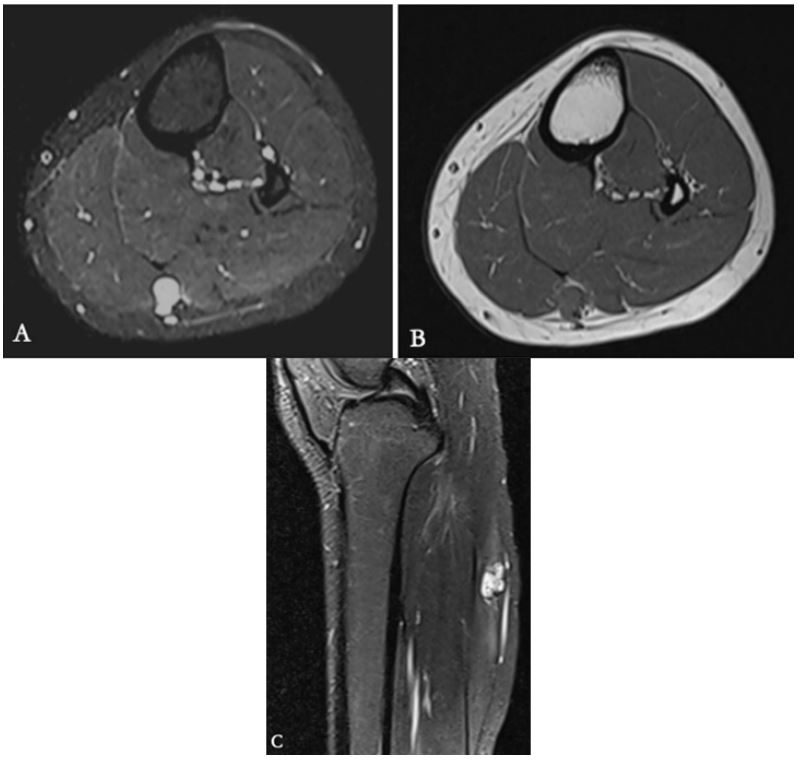
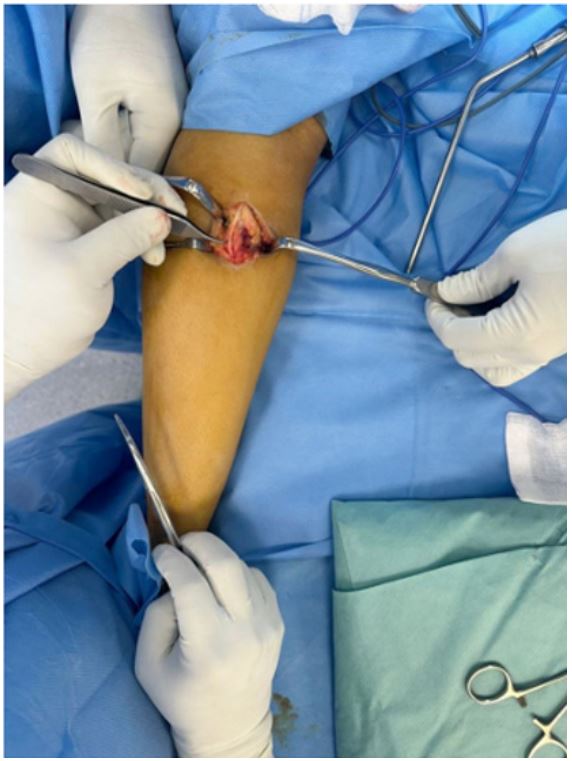
Case 2: A 15 year old girl presenting with pain and swelling in the calf for a year. Pain was aggravated by walking, squatting and sitting cross-legged. On examination, ullness was present over the calf and pain was elicited on passive dorsiflexion of the ankle. Imaging revealed a soft tissue lesion, in the intermuscular location between the medial and lateral head of gastrocnemius, with hyperintense T2 signal, low intensity foci suggesting phleboliths and proliferating fatty component (Figures 3 and 4). Complete surgical excision was carried out (Figure 5). Histopathology revealed fibrocollagenous tissue with thin-walled markedly dilated and congested vessels of varying calibre, and few clusters of adipocytes - features consistent with FAVA.
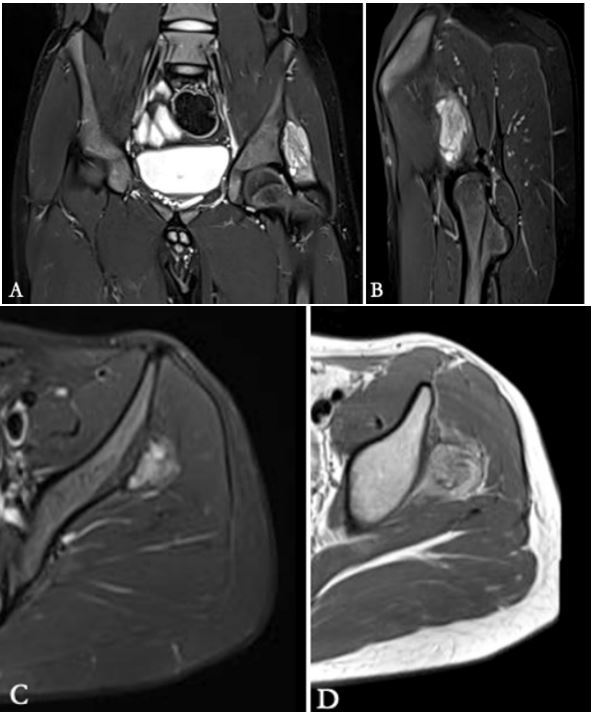
Case 3: A 14 year old boy presenting with left hip pain for 3 years after trivial trauma to the site. Pain was slowly progressive, and followed by limping and constant pain for 1 year. There was no associated limitation of daily activities. On clinical examination, there was wasting of the thigh and tenderness in the gluteal region. MRI (Figure 6) showed a focal intramuscular heterogenous lesion involving the gluteus minimus. The child underwent complete excision of the lesion and gluteus minimus and histopathological findings were consistent with FAVA.

Discussion
Fibro-adipose vascular anomaly is a relatively novel complex mesenchymal disorder, essentially implying a slow flow vascular malformation with dense fibrous and adipose elements within. Most common presentation is a painful limb with dysfunction (contracture) [1]. It has a propensity for extremity involvement, particularly the calf and forearm and the degree of muscular involvement correlates with severity of symptoms. Before even beginning the clinical examination of a child presenting with extremity pain and dysfunction, the key feature of FAVA is that the overlying skin is normal. This helps exclude hemangioma (which has been historically a close differential for FAVA before it was separately described), as well as venous malformations which have distinct skin features. Muscle involvement in FAVA can be focal or diffuse, and the imaging and histopathological features reflect the underlying anomalous veins intertwined with fibrofatty tissue [1]. Phlebectasia is characteristic of FAVA and can be within the involved muscle or adjacent subcutis [1]. Imaging diagnosis of FAVA usually employs a combination of ultrasound and MRI complementing each other to make a definitive impression. FAVA is commonly seen as a solid, heterogeneous echogenic lesion replacing the normal fibrillary pattern of muscle [1], with absence of arterial flow and occasional small venous pockets. MRI better delineates the solid component with phlebectasia [1] and T1 bright areas suggesting fatty components. Plain radiographs can occasionally show adjacent cortical irregularity or calcifications within the lesion. Close imaging differentials include intramuscular hemangiomas, slow flow venous malformations and syndromic vascular malformations such as PTEN associated soft tissue hamartomas. Venous malformations predominantly involve the quadriceps (Figure 7) and intrinsic muscles of the foot [1] while FAVA most commonly involves the gastrocnemius [1]. VMs do not show significant solid components on imaging, and have a typical compressible stagnant blood pool that is seen on both ultrasound and MRI. Clinical features may further help distinguish these two entities - children with VM present with episodic pain triggered by clots and engorgement, while those having FAVA usually present with constant, severe pain and contractures [1]. It can sometimes be difficult to differentiate intramuscular hemangiomas from FAVA on imaging. Characteristic imaging features of hemangiomas include phleboliths on radiographs/ultrasound and MRI, along with multiple flow voids seen on MR images. These are seen as intense vascularity on doppler images. Fatty hypertrophy may be seen on T1 weighted images, quite similar to FAVA. Differentiation can be aided by phleboliths and bony changes seen with hemangiomas, such as adjacent periosteal reaction, coarsening of bony trabeculae and reactive sclerosis [6]. Hemangiomas also show typical overlying skin discoloration, and intense post contrast enhancement on MRI. It is pertinent to determine the diagnosis of FAVA to guide appropriate management strategy that may include surgical excision with or without sclerotherapy, and release of the joint contractures.
Conclusion
The management of vascular malformations may be complicated by ambiguous clinical and imaging findings, further amplified by evolving terminology. Morphological characteristics of the lesion that can be defined on imaging, as described above can help pertinent decisions such as surgical excision versus sclerotherapy or a combined approach, to help achieve maximum symptom relief while retaining limb function and range of motion.
References
- Alomari AI, Spencer SA, Arnold RW, Chaudry G, Kasser JR, Burrows PE, et al. Fibro-Adipose Vascular Anomaly: Clinical-Radiologic-Pathologic Features of a Newly Delineated Disorder of the Extremity. Journal of Pediatric Orthopaedics. 2014; 34(1): 109- 17.
- Merrow AC, Gupta A, Patel MN, Adams DM. 2014 revised classification of vascular lesions from the International Society for the study of vascular anomalies: Radiologic-pathologic update. Radiographics 2016; 36(05): 1494-1516.
- Available at. https://www.issva.org/UserFiles/file/ISSVA- Classification-2018.pdf.
- Amarneh, M, Shaikh, R. Clinical and imaging features in fibroadipose vascular anomaly (FAVA). Pediatr Radiol. 2020; 50: 380- 387. https://doi.org/10.1007/s00247-019-04571-6.
- Khera PS, Garg PK, Babu S, Elhence P, Tiwari S, Nk S. Fibro Adipose Vascular Anomaly: A Rare and Often Misdiagnosed Entity. Indian J Radiol Imaging. 2021; 31(03): 776-81.
- Pattamapaspong N, Peh WC, Shek TW. Imaging of intramuscular haemangiomas of the extremities. Singapore Med J. 2020; 61(3): 122-128. doi: 10.11622/smedj.2020030. PMID: 32488279; PMCID: PMC7905120