
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Persistent hyperprolactinemia in a patient with secondary “empty sella” as a predictive factor of disease relapse
Flavia Urbano1*; Luigi Antonio Moscogiuri1 ; Mariantonietta Francavilla2 ; Maria Felicia Faienza3
1University Pediatric Unit, Giovanni XXIII Pediatric Hospital, Bari, Italy.
2Radiology Department, Giovanni XXIII Pediatric Hospital, Bari, Italy.
3Pediatric Unit, Department of Precision and Regenerative Medicine and Ionian Area, University of Bari “Aldo Moro”, Bari, Italy.
*Corresponding Author: Flavia Urbano
University Pediatric Unit, Giovanni XXIII Pediatric Hospital, Bari, Italy.
Email: flaviaurbano84@gmail.com
Received : Jan 01, 2024
Accepted : Feb 07, 2024
Published : Feb 14, 2024
Archived : www.jclinmedimages.org
Copyright : © Urbano F (2024).
Abstract
Pituitary adenomas, recently renamed Pituitary Neuroendocrine Tumors (PitNET), are benign neoplasms of the adenohypophysis. Among them, prolactinoma represents the most common form. We report a case of hyperprolactinemia initially attributed to pituitary macroadenoma (prolactinoma), with consequent appearance of “empty sella” attributable to apoplexy of the lesion and subsequent release of the neoplasm preceded by a progressive and constant elevation of serum Prolactin (PRL) level unresponsive to dopamineagonist treatment. Follow up with brain MRI allowed the early identification of a new pituitary lesion and, consequently, the prevention of potential locoregional complications. The patient underwent endoscopic transphenoidal excision of the mass. The histological examination confirmed the diagnosis of PitNET with granulomatous infiltration. Our case highlights the relationship between PRL values and prolactinoma volume. Hyperprolactinemia in a patient with “empty sella” is usually modest, therefore an increase in serum PRL level that is unresponsive to pharmacological treatment with dopamine analogues, even in case of negative brain imaging, should suggest the persistence of residues of abnormal cells with aberrant PRL production.
Citation: Urbano F, Moscogiuri LA, Francavilla M, Faienza MF. Persistent hyperprolactinemia in a patient with secondary “empty sella” as a predictive factor of disease relapse. Open J Clin Med Images. 2024; 4(1): 1164.
Introduction
Pituitary adenomas, also called pituitary Neuroendocrine Tumors (PitNET), are benign neoplasms of the adenohypophysis [1]. Among them, prolactinoma represents the most common form, although it is rare in pediatric age with an estimated incidence of 0.1 per 1,000,000 inhabitants [2]. Prolactinoma is classified according to its size in microprolactinoma (max diameter <1 cm) and macroprolactinoma (max diameter >1 cm). It rarely grows larger than 4 cm and it is called giant prolactinoma [3]. Microprolactinoma has a low tendency to proliferate and rarely it has a poor prognosis, while macroprolactinoma proliferates more easily and deserves a careful follow up [4]. The Prolactin (PRL) secretion is usually mediated by physiological stimuli as breastfeeding, pregnancy, stress (including venipuncture), physical exercise [5]. However, sometimes an abnormal production of PRL can be observed. PRL release is also under the inhibitory control by dopamine, a peptide hormone released by the hypothalamus. Dopamine blocks PRL release by acting on the Dopamine Receptors (D2R) [6]. For this reason, any pathological process that breaks down the link between these systems at the pituitary stalk could lead to an increase in PRL levels, that is generally quite modest (up to six times the normal reference values). The use of drugs can also lead to a blockade of dopamine release receptors, resulting in an increase in PRL as well [7]. A rare cause of increase in PRL levels is the lymphocytic hypophysitis, an autoimmune disorder that is responsible for a severe glandular inflammation. In this case, the measurement of Anti-Pituitary Antibodies (APA) is useful [8].
PRL levels are usually closely related to the size of the prolactinoma [9]. Therefore, a new elevation of PRL after a reduction phase could correlate with a disease relapse, making it necessary to carry out instrumental investigations. High levels of PRL stimulate the mammary gland to promote lactogenesis, therefore one of the most common symptoms is galactorrhea. PRL values should be measured in all patients with non-physiological galactorrhea [10]. There is an inverse relationship between PRL and Gonadotropin-Releasing Hormone (GnRH): when PRL is elevated, it acts by suppressing the GnRH release presumably through the blockade of kisspeptinergic hypothalamic neurons [9]. Consequently, this hormonal effect causes primary or secondary amenorrhea, menstrual irregularities, infertility, decreased libido, erectile dysfunction in males, including hypogonadotropic hypogonadism [11]. In the presence of a pituitary adenoma, it is essential to consider possible deficits in the release of other pituitary trophins: Thyrotropin-Releasing Hormone (TSH), Growth Hormone (GH), Adrenocorticotropic Hormone (ACTH). In relation to the close relationship between the pituitary gland and the optic chiasm, patients diagnosed with pituitary adenoma should perform a visual field test. Magnetic Resonance Imaging (MRI) with contrast agent (gadolinium) is considered the gold standard for the study of the hypothalamicpituitary region [12]. Large adenomas, especially if associated to rapid growth, can lead to a process known as pituitary apoplexy [13]. It is a hemorrhagic infarction of the pituitary region whose reabsorption can lead to a radiological condition known as “empty sella” [14].
The term “empty sella” indicates a radiological appearance in which the sella turcica appears devoid of the pituitary gland, with associated herniation of the subarachnoid space within the sella. The pituitary gland will appear crushed and compressed towards the sellar floor. This radiological condition may be primary (if an underlying cause cannot be established) or secondary (e.g. surgery, radiotherapy, regression of pituitary adenomas). In the “empty sella” condition, if the pituitary stalk is compressed, the release of dopamine from the pituitary gland may also be deficient, leading to a loss of the dopaminergic inhibition on the pituitary PRL-secreting cells and secondary abnormal increase in PRL secretion [15].
The treatment of prolactinoma is based on medical and surgical therapy. Medical therapy is based on the use of dopamine agonists (bromocriptine, cabergoline). Cabergoline is the most used and well tolerated drug. The goal of the therapy is to treat the symptoms of the disease, to reduce the PRL, and finally to contract the volume of the adenoma. The usually recommended dosage varies from 0.5 mg to maximum 3.5-4 mg per week [16]. According to Lee et al. [17] the initial response to dopamine analogues predicts the evolution of the disease; a significant reduction in the volume of the adenoma (>25%) after three months of pharmacological therapy indicates an adequate longterm response. Medical therapy should be discontinued after two years in the absence of a pituitary mass visible on MRI and with normal serum PRL levels [9,18]. The most used approach is to gradually reduce the dose of cabergoline. A new increase in serum PRL levels after suspension requires the performance of a brain MRI due to the risk of persistence of disease.
We report a case of a girl affected with hyperprolactinemia initially attributed to pituitary macroadenoma (prolactinoma), with consequent appearance of “empty sella” attributable to apoplexy of the lesion, and subsequent reappearance of the neoplasm preceded by a progressive and constant elevation of PRL levels, unresponsive to dopamine-agonist treatment.
Case presentation
A 14 years and 6 months old female came to our observation for a history of vomiting, photophobia and persistent headache. Admitted to “Giovanni XXIII” Hospital in Bari, the patient underwent a brain MRI which identified a “solid formation relating to the intra- and supra-sellar adenohypophyseal extension (diameter 20x18 mm) with deviation to the right of the pituitary stalk and partial elevation of the optic chiasm, consistent with macroadenoma”.
At clinical examination she presented with normal pubertal development (B3, PH4) and normal growth. Absence of menarche.
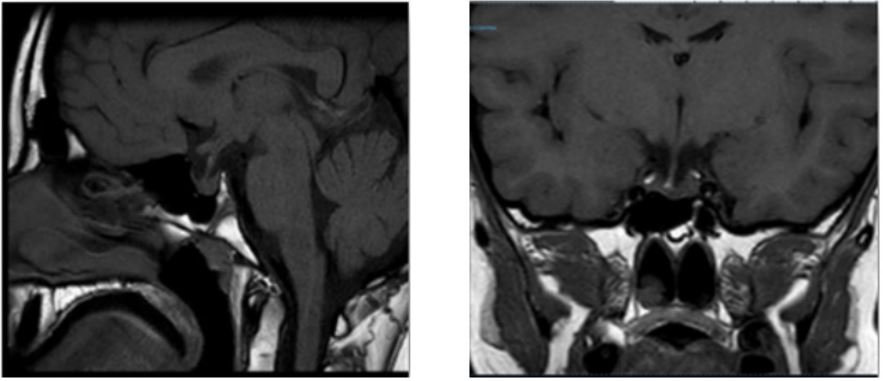
Visual field examination was normal. Serum PRL levels were >100 ng/mL (normal values: 6.2-23.4). Therefore, therapy with cabergoline at the dosage of 0.5 mg/week was started, and subsequently increased to 1 mg/week due to the further elevation of PRL level. After 3 months, a new MRI showed a significant reduction of the adenoma (4x2 mm), and a normalization of PRL levels (11.23 ng/ml) was observed. After further 6 months a new increase in PRL levels (56 ng/ml) was found, in the absence of any symptoms except for the persistence of absence of menarche. The brain MRI (Figure 1) showed an “empty sella” with a minimum thickness of the pituitary parenchyma of 2 mm, compressed on the bottom of the sella with pituitary stalk in place.
For the persistence of primary amenorrhea, a test with triptorelin was carried out that revealed a response consistent with hypogonadotropic hypogonadism. Pelvic ultrasound showed an involution of the uterus and of the ovaries to a prepubertal volume. PRL presented a progressive increase from 86 ng/ml to 1050 ng/ml, despite the increase in cabergoline dosage up to 2 mg/week. Macroprolactin, thyroid and adrenal function were normal.
The persistence of high PRL levels was initially interpreted as a disruption of the pituitary stalk secondary to the involution of the adenoma, with consequent loss of the inhibitory dopaminergic tone on PRL-secreting cells.
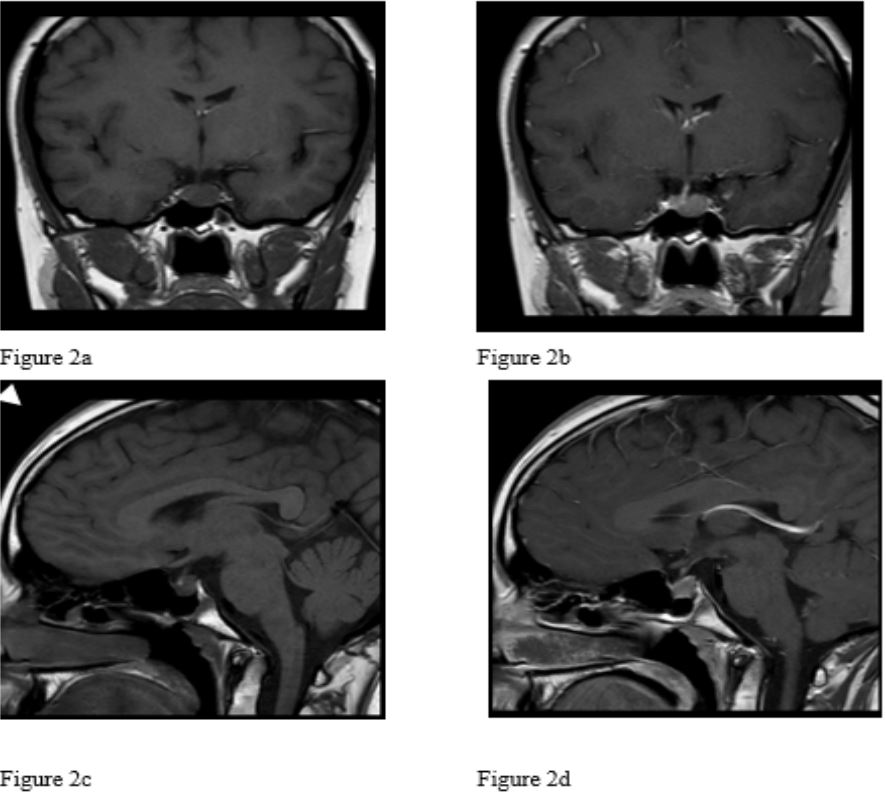
Two years and 8 months after the diagnosis of secondary “empty sella”, a new brain MRI (Figure 2) showed a pituitary lesion (maximum size 11 mm) which caused underlevelling of the left portion of the sellar floor and downward dislocation of the neurohypophysis, consistent with the diagnosis of pituitary adenoma. The patient underwent successful endoscopic transsphenoidal excision. The histological examination confirmed the diagnosis of PitNET with granulomatous infiltration.
Discussion
We presented a case of pituitary adenoma with a peculiar and unexpected clinical evolution. After the first diagnosis of macroadenoma, pharmacological treatment for three months with cabergoline at a dosage of 1 mg/week allowed a significant reduction of the neoplasm, until its complete involution and normalization of PRL levels. Subsequently, the brain MRI showed an “empty sella” secondary to apoplexy of the adenoma. Secondary empty sella is related to various pathological processes of the sellar region including apoplexy of a pituitary adenoma. Hyperprolactinemia is generally mild (<50 ng/ml) and is present in 10% of subjects [14,15].
In the following months, the slow and gradual increase in serum PRL levels, in the absence of adenohypophyseal lesions compatible with prolactinoma, required increasing dopamine agonist therapy. In the first hypothesis, the elevation of the PRL level was attributed to the interruption of the pituitary stalk secondary to the involution of the adenoma with consequent loss of the inhibitory dopaminergic tone on prolactin-secreting cells. The lack of response to treatment with high-dose cabergoline (2 mg/week), and the progressive and constant increase in serum PRL levels did not explain the loss of dopaminergic inhibitory influence alone. For this reason, the patient underwent a close follow-up with MRI, with evidence of a new formation attributable to prolactin-secreting macroadenoma, approximately 2 years and 6 months after the first diagnosis.
It is rarely described that a prolactinoma that responds adequately to low doses of cabergoline relapses upon suspension; in most of the cases described they can be successfully treated with a pharmacological rechallenge [9]. In these circumstances it is advisable to increase medical treatment up to the maximum dosage allowed. In our patient, the maximum drug dosage was neither helpful in reducing the serum PRL level, nor in preventing the development of a pituitary mass visible on MRI. The recurrence of the adenoma presented characteristics of greater “refractoriness” to treatment, for this reason it was necessary to undertake excisional surgical treatment of the lesion. Hypogonadotropic hypogonadism has been treated with estrogen-progestin therapy (estradiol and nomegestrol) with regularization of menstrual cycles. It is known that estrogens increase PRL levels, therefore cabergoline should not be suspended for the duration of treatment with oral contraceptives. Studies on the role of oral contraceptives and the development of prolactinoma are controversial [19,21]. In cases of relapse of “refractory” disease, as in our case, the greatest concern is the risk of carcinoma [1,22].
Conclusion
In the case described, our patient developed a macroprolactinoma that at the beginning responded brilliantly to low doses of cabergoline. The apoplexy of the lesion led to a secondary “empty sella” with subsequent increase in PRL levels. Follow up with brain MRI allowed the early identification of a new pituitary lesion and, consequently, the prevention of potential locoregional complications.
Our case highlights the relationship between PRL values and prolactinoma volume. Hyperprolactinemia in a patient with “empty sella” is usually modest, therefore an increase in serum PRL level that is not responsive to pharmacological treatment with dopamine analogues, even in case of negative brain imaging, should suggest the persistence of residues of abnormal cells with aberrant PRL production.
References
- Trouillas J, Jaffrain-Rea ML, Vasiljevic A, Raverot G, Roncaroli F, et al. How to Classify the Pituitary Neuroendocrine Tumors (PitNET)s in. Cancers (Basel). 2020; 12(2): 514.
- Yang A, Cho SY, Park H, Kim MS, Kong DS, et al. Clinical, Hormonal, and Neuroradiological Characteristics and Therapeutic Outcomes of Prolactinomas in Children and Adolescents at a Single Center. Front Endocrinol (Lausanne). 2020; 4: 11-527.
- Yatavelli RKR, Bhusal K. Prolactinoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2023.
- P Iglesias, JJ Díez, Macroprolactinoma: A diagnostic and therapeutic update, QJM: An International Journal of Medicine. 2013; 495-504.
- Levine S, Muneyyirci-Delale O. Stress-Induced Hyperprolactinemia: Pathophysiology and Clinical Approach. Obstet Gynecol Int. 2018; 3: 9253083.
- Flückiger E. Dopaminergic control of prolactin secretion. Bull Schweiz Akad Med Wiss. 1978; 34(1-3): 191-6.
- Petty RG. Prolactin and antipsychotic medications: Mechanism of action. Schizophr Res. 1999; 1: 35 S67-73.
- Faje A. Hypophysitis: Evaluation and Management. Clin Diabetes Endocrinol. 2016; 6: 2-15.
- Petersenn S, Fleseriu M, Casanueva FF, Giustina A, Biermasz N, et al. Diagnosis and management of prolactin-secreting pituitary adenomas: A Pituitary Society international Consensus Statement. Nat Rev Endocrinol. 2023; 19(12): 722-740.
- Sakiyama R, Quan M. Galactorrhea and hyperprolactinemia. Obstet Gynecol Surv. 1983; 38(12): 689-700.
- Irfan H, Shafiq W, Siddiqi AI, Ashfaq S, et al. Prolactinoma: Clinical Characteristics, Management and Outcome. Cureus. 2022; 14(10): e29822.
- Melmed S. Pituitary-Tumor Endocrinopathies. N Engl J Med. 2020; 382(10): 937-950.
- Biagetti B, Simò R. Pituitary Apoplexy: Risk Factors and Underlying Molecular Mechanisms. Int J Mol Sci. 2022; 23(15): 8721.
- Nomura K, Kono A, Ujihara M, Masuda A, et al. Pituitary adenoma results in the empty sella syndrome. Jpn J Med. 1989; 28(5): 625-7.
- Aruna P, Sowjanya B, Reddy PA, Krishnamma M, Naidu JN. Partial empty sella syndrome: A case report and review. Indian J Clin Biochem. 2014; 29(2): 253-6.
- Inder WJ, Jang C. Treatment of Prolactinoma. Medicina (Kaunas). 2022; 58(8): 1095.
- Lee Y, Ku CR, Kim EH, Hong JW, Lee EJ, et al. Early prediction of long-term response to cabergoline in patients with macroprolactinomas. Endocrinol Metab (Seoul). 2014; 29(3): 280-92.
- Xia MY, Lou XH, Lin SJ, Wu ZB. Optimal timing of dopamine agonist withdrawal in patients with hyperprolactinemia: a systematic review and meta-analysis. Endocrine. 2018; 59(1): 50-61.
- Vaisrub S. Pituitary prolactinoma and estrogen contraceptives. JAMA. 1979; 242(2): 177-8.
- Maheux R, Jenicek M, Cleroux R, Beauregard H, De Muylder X, et al. Van Campenhout J. Oral contraceptives and prolactinomas: a case-control study. Am J Obstet Gynecol. 1982; 143(2): 134-8.
- Testa G, Vegetti W, Motta T, Alagna F, Bianchedi D, et al.Twoyear treatment with oral contraceptives in hyperprolactinemic patients. Contraception. 1998; 58(2): 69-73.
- Guaraldi F, Zoli M, Righi A, Gibertoni D, Marino Picciola V, et al. A practical algorithm to predict postsurgical recurrence and progression of pituitary neuroendocrine tumours (PitNET)s. Clin Endocrinol (Oxf). 2020; 93(1): 36-43.