
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Missed foreign body falsely interpreted as glass in surgery
Jakob Hama1*; Daniel Contractor2
1Internal Medicine, New York City Health and Hospitals, Queens Hospital Center, 82-68 164th St, Queens, NY 11432, USA.
2Interventional Radiology, New York City Health and Hospitals, Queens Hospital Center, 82-68 164th St, Queens, NY 11432, USA.
*Corresponding Author: Jakob Hama
Internal Medicine, New York City Health and Hospitals,
Queens Hospital Center, 82-68 164th St, Queens, NY
11432, USA.
Email: hamaj@nychhc.org
Received : Feb 02, 2024
Accepted : Feb 04, 2024
Published : Mar 11, 2024
Archived : www.jclinmedimages.org
Copyright : © Hama J (2024).
Abstract
Retained Foreign Bodies (FBs) in soft tissues are typically a complication of open wounds from trauma, accidents, and surgery, for which plenty of patients seek acute medical care. The importance of localizing these FBs is vital to patient health because it reduces the detrimental complications of loss of function, local tissue damage, infection, and sepsis. In today’s modern age, many automobile taillights are composed of three components: the polycarbonate outer shell, the light bulb, and various metal casings. Occasionally, patients present with one of these objects retained in their body. Here, we present the case of a FB that was dictated as a hematoma; however, it was a piece of polycarbonate that was reported as a piece of glass in the operating room transcript. Based upon imaging a piece of taillight polycarbonate at our institution, the Hounsfield Units (HU) averaged to be 88.62. Nonetheless, if there is acute blood in soft tissues, taillight plastic could be an appropriate differential; however, a hematoma is less likely to be polycarbonate from car rear lights based on the HU.
Keywords: Foreign body; Left knee; Extra articular; Infection.
Abbreviations: FB: Foreign Body; ED: Emergency Department; XRay: Radiograph; CT: Computed Tomography; US: Ultrasonography; MRI: Magnetic Resonance Imaging.
Citation: Hama J, Contractor D. Missed foreign body falsely interpreted as glass in surgery. Open J Clin Med Images. 2024; 4(1): 1170.
Introduction
Patients commonly seek medical care either at the primary medicine clinic or the Emergency Department (ED) for Foreign Bodies (FBs) in the soft tissues of the extremities. Presentations can range from trauma, accidents, falls, lacerations, and recent surgical procedures. In addition to treating the acute incident and identifying obvious FBs wedged into the underlying tissue, it is important to keep suspicion high for FBs because, depending on the imaging modality and material composition, the FB may be missed or diagnosed as another disease process or medical device.
Accidents involving motor vehicles contribute to a significant amount of healthcare-related presentations (11.6 ED visits per 1,000 people per year) [1]. Motor vehicle lights are composed of a polycarbonate external casing/cover, a bulb made of glass, and metal filament components in the casing holding the light bulb. Computed Tomography (CT) is a wonderful imaging modality to differentiate these three mediums and locate the anatomic position of these FBs in relation to vital structures. However, the Hounsfield Units (HU) of glass and metal are distinct from other structures (Table 1); plastic is not and could be interpreted as acute blood.
Here, we present the case of a FB that was originally dictated as a hematoma on the initial CT scan; this patient developed septic arthritis, and during debridement, the operating room transcript described the FB as a piece of auto glass. This case report addresses how the FB was a piece of polycarbonate based on HU; a differential of hematoma is less likely, and when diagnosing a FB, actively consider taillight plastic.
Case presentation
A 54-year-old presented to the ED because of a fall and concomitant alcohol intoxication. Upon eliciting a further history, the patient described that he was riding his bicycle when he got cut off by a car, his left knee slammed into the back of a car’s taillight, and the taillight shattered, which caused a laceration on the lateral side of his left knee. Physical exam was significant for left knee swelling with a 3x1 cm crescent laceration over the left lateral knee. The prepatellar region was boggy, and there was active bleeding from the laceration. The rest of the neurological and musculoskeletal exam was within normal limits.
Conventional x-rays were ordered of the femur, knee, tibia, and fibula, all revealing no acute osseous abnormality (Figure 1). Specifically, the CT knee demonstrated “no acute fracture or dislocation. No osseous erosive process. No significant knee effusion. Small amount of soft tissue air, likely due to injury in the prepatellar soft tissues, correlate clinically. Small hyperdensity is seen anterior to the patella likely due to small hematoma measuring 1 cm x 0.5 cm with prepatellar soft tissue swelling” (Figure 2).
Two and a half weeks later, the patient presented to the ED with left knee pain, fever, tachycardia and endorsed that he fell on the left knee two days ago. Repeat non-contrast CT of the left knee was dictated as “small quadrangular density projecting within the soft tissues anterolateral to the patella unchanged from prior exam and may represent a small foreign body. This measures 1.6 cm in diameter” (CT knee). Orthopedic surgery was consulted in the ED and scheduled for the patient for exploration of the wound and left lower extremity removal of foreign body knee irrigation. In the operating room, a 2 cm x 0.5 cm piece of “glass” was found.
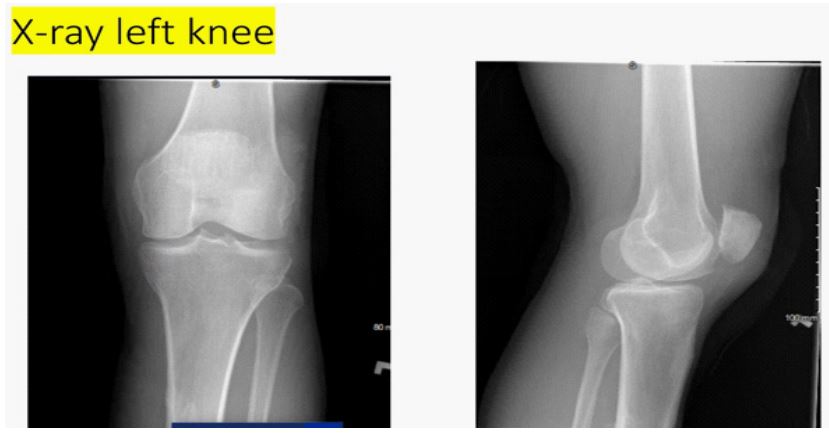
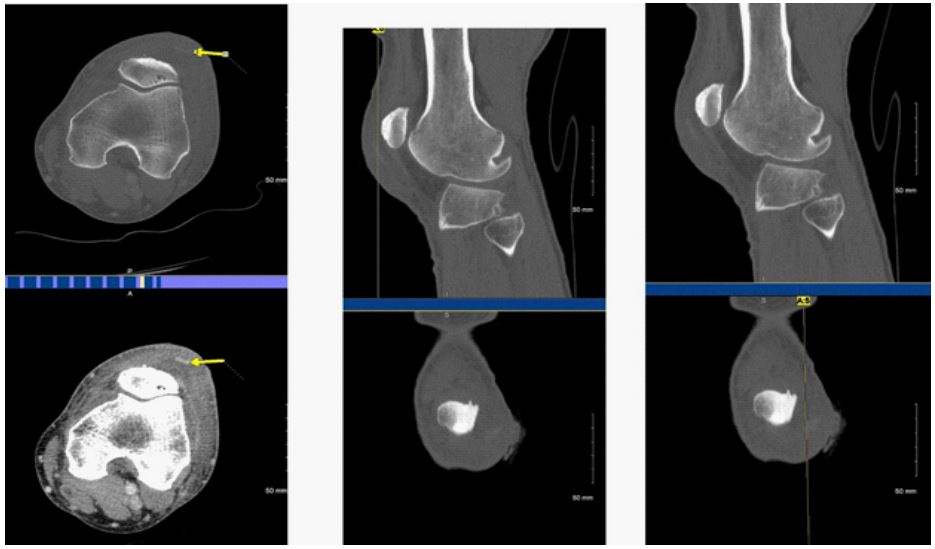
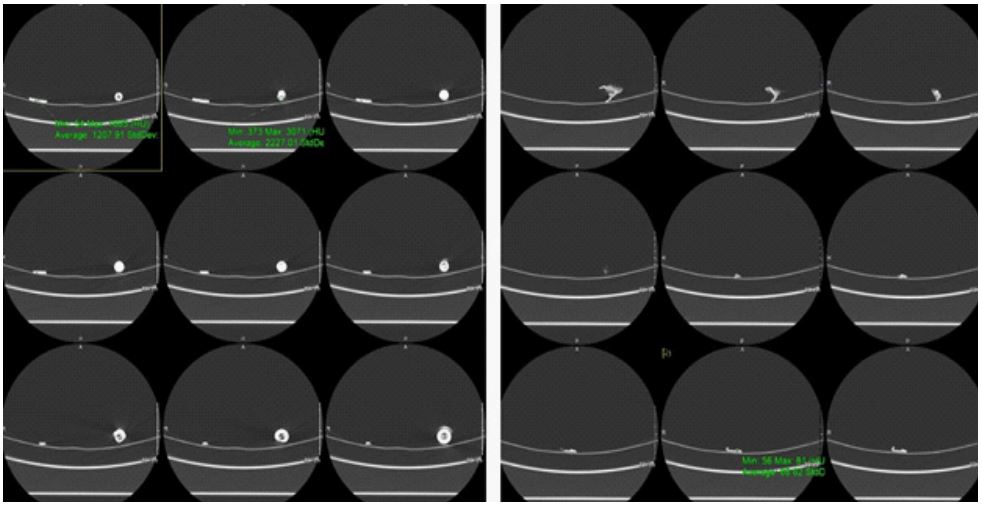
Table 1:Hounsfield Units (HU) of various densities of sub- stances that may be found in the human body.
| Air | -1000 (Herring 2019) |
|---|---|
| Fat | -100- -40 (Herring 2019) |
| Water | 0 (Herring 2019) |
| Soft tissue | 20-100 (Herring 2019) |
| Blood (unclotted, clotted, hematoma) | 40-60 (Zech 2014) |
| Blood extravasation | 91-274 (Singh 2017) [9] |
| Plastic |
10-100 (Alfuraih 2022, Carneiro et al. 2020) [5,6] |
| Glass | 500-2700 (Tseng 2015) [2] |
| Metal (except aluminum) | >3000 (Tseng 2015) [2] |
Discussion
Identifying FBs the first time, before complications arise, is of utmost importance for patient outcomes. Choosing the right imaging exam is crucial because each imaging modality has its limitations for visualizing the FB. The composition of the FB determines how they are identified based on the imaging modality. For the purposes of this case report, we will focus on the potential retained foreign bodies associated with taillight components, which are plastic, glass, and metal. When x-rays are obtained, plastic is radiolucent, and metal and glass are radiopaque except for thin aluminum [2]. On ultrasound, all three modalities have hyperechoic structures with posterior reverberation [3]. With CT, the plastic range of Hounsfield units is 10-100 (Table 1), glass is 500-1900, and metal is >3000 (Table 1). MRI, metal demonstrates magnetic susceptibility artifact, glass, and plastic has low signal intensity at T1W1 and T2W1 [3].
Typically, x-rays are the first imaging study ordered when a foreign body is suspected for two reasons. First, x-rays are widely available, the cost is low, and there is minimal radiation exposure to the patient. Second, they are sensitive, especially in detecting radiopaque mediums, where the sensitivity of picking up FBs in these mediums was reported as 98% [4]. The drawbacks of x-rays are that it has poor contrast between soft tissues and nonradiopaque objects, as they blend into soft tissues and are hard to identify. If computed radiography is nondiagnostic, US is the next best step because all foreign bodies can be identified with it [5,6]. Ultrasound is the next best step because, like x-ray, it is widely available, relatively inexpensive, and has no ionizing radiation exposure to the patient. US does have weaknesses, such as how deep the fb is (depths >4 cm may be difficult to visualize), the position/alignment of the transducer, and false negatives with other concomitant pathology (hematomas or anything creating a hyperechogenic structure) [3]. If ultrasound is nondiagnostic, CT is the next best step, especially for non-biodegradable FBs. The benefits of CT are the ability to see FBs visualized at deeper depths, localize FB in relation to sensitive structures (blood vessels, nerves), and better contrast between tissue densities and measuring Hounsefield units of the objects. The negatives of CT are that it is expensive, has significant ionizing radiation exposure, and may not display superficial FBs. MRI is another modality used to detect FBs; however, there is limited research on it; it’s expensive, time-consuming, and not widely available. The tissue differentiation is by far the most impressive on MRI (unless the FB is metallic), especially for soft tissue FBs.
Based on the case presented above, the FB was missed on plain film (Figure 1) and recognized on the CT scan (Figure 2) but dictated as a small hematoma. This is a common theme; a study done in vitro demonstrated that no reader could visualize plastic on x-ray, but could identify glass and metal [5]. This finding was further corroborated by [6] using their pig phantom model, 2 out of 5 (different types of plastic) were visible on conventional x-rays. The reason is that radio-opacity is related to atomic number. Plastic is made of hydrogen, carbon, oxygen, and fluorine; depending on the composition, the atomic number ranges from 5.44-8.43 [7]. Soft tissue has an atomic number of roughly 7.5; because the difference between the atomic numbers is negligible, there is no contrast between the mediums, which makes neither medium differentiated from the other in plain radiography [8]. In contrast, the atomic number of metal is significantly greater than that of soft tissue; it is radiopaque and is clearly differentiated from soft tissue.
Regarding CT findings, plastic can range from 10-100 in most studies (Table 1). Plastic from an automobile light in the CT scanner at our medical center had a HU of 88.62 (Figure 3), and the study was dictated as a hematoma. A hematoma usually has a HU of 40-60 (Table 1); depending on the onset (acute or chronic), the HU can range from 28-82 [9] because of the difference in calcium and iron based on the time. Identifying that car taillight plastic averagely attenuates at 88.62 HU at our institution highlights an area of improvement that hematoma should not have been suggested. The purpose of this case is to prevent further deleterious events from happening in the future. Based on the medical record, a piece of glass was pulled out of the surgical wound, this is not probable because glass has substantially higher attenuation than plastic on CT (Table 1). In addition, if the FB was glass, it would have likely been easily identifiable on x-ray due to the radio-opacity of glass.
Conclusion
In conclusion, we presented a case of a missed retained foreign body that was called a piece of auto glass in surgery, but based upon radiological findings, is a piece of automobile taillight polycarbonate that was dedicated as a hematoma. Highlighting the importance of knowing that taillight auto glass attenuates at around 88 HU.
References
- Davis D, Cairns, C. (2023). Emergency Department Visit Rates for Motor Vehicle Crashes by Selected Characteristics: United States, 2019-2020. NCHS Data Brief, 466, 1-8. https://www.ncbi.nlm.nih.gov/pubmed/37093616
- Tseng, H.-J., Hanna, T. N., Shuaib, W., Aized, M., Khosa, F., & Linnau, K. F. (2015). Imaging Foreign Bodies: Ingested, Aspirated, and Inserted. Annals of Emergency Medicine, 66(6), 570-582.e5. https://doi.org/10.1016/j.annemergmed.2015.07.499
- Carneiro, B. C., Cruz, I. A. N., Chemin, R. N., Rizzetto, T. A., Guimarães, J. B., Silva, F. D., Junior, C. Y., Pastore, D., Ormond Filho, A. G., & Nico, M. A. C. (2020). Multimodality Imaging of Foreign Bodies: New Insights into Old Challenges. Radiographics: A Review Publication of the Radiological Society of North America, Inc, 40(7), 1965-1986. https://doi.org/10.1148/rg.2020200061
- Manthey, D. E., Storrow, A. B., Milbourn, J. M., & Wagner, B. J. (1996). Ultrasound versus radiography in the detection of softtissue foreign bodies. Annals of Emergency Medicine, 28(1), 7-9. https://doi.org/10.1016/s0196-0644(96)70130-0
- Alfuraih, A. M., Almutairi, F. N., Alotaibi, S. B., & Alshmrani, A. A. (2022). Semi-quantitative scoring of imaging modalities in detecting soft tissue foreign bodies: an in vitro study. Acta Radiologica, 63(4), 474-480. https://doi.org/10.1177/0284185121999654
- Ingraham, C. R., Mannelli, L., Robinson, J. D., & Linnau, K. F. (2015). Radiology of foreign bodies: how do we image them? Emergency Radiology, 22(4), 425-430. https://doi.org/10.1007/s10140-015-1294-9
- Phelps, M. E., Gado, M. H., & Hoffman, E. J. (1975). Correlation of effective atomic number and electron density with attenuation coefficients measured with polychromatic x rays. Radiology, 117(3 Pt 1), 585-588. https://doi.org/10.1148/117.3.585
- Pinto, A., Sparano, A., & Tecame, M. (2014). Soft Tissue Foreign Bodies. In A. Pinto & L. Romano (Eds.), Imaging of Foreign Bodies (pp. 105-113). Springer Milan. https://doi.org/10.1007/978-88-470-5406-6_11
- Singh, A. (2017). Emergency Radiology: Imaging of Acute Pathologies. Springer. https://play.google.com/store/books/details?id=isY7DwAAQBAJ.