
Open Journal of
Clinical and Medical Images
Short Report - Open Access, Volume 4
Ruptured splenic abscess with pneumoperitoneum secondary to chronic pyelonephritis
Hutton White1; Jacob Schaub1; Kyle Moehlin1; Michael Kopka2; Erica Roach2; Tarik Wasfie1*
1Clinical Professor of Surgery, MSU COM and CMU-Medical School Core Faculty, Surgical Residency Program, Ascension Genesys Hospital, Grand Blanc, Michigan 48439, USA.
2Medical Student, Central Michigan University College of Medicine, Michigan State University College of Osteopathic Medicine, Michigan 48439, USA.
*Corresponding Author: Tarik Wasfie
Clinical Professor of Surgery, MSU COM and CMU-Medical School Core Faculty, Surgical Residency Program,
Ascension Genesys Hospital, Grand Blanc, Michigan
48439, USA.
Tel: 810-853-9900;
Email: twasfie@gmail.com
Received : Feb 05, 2024
Accepted : Feb 07, 2024
Published : Mar 14, 2024
Archived : www.jclinmedimages.org
Copyright : © Wasfie T (2024).
Abstract
Keywords: Splenic abscess; Pneumoperitoneum; Surgical management.
Citation: White H, Schaub J, Moehlin K, Kopka M, Wasfie T, et al. Ruptured splenic abscess with pneumoperitoneum secondary to chronic pyelonephritis. Open J Clin Med Images. 2024; 4(1): 1171.
Background
Splenic abscesses are relatively uncommon occurrences with autopsy studies estimating the incidence to be between 0.2% to 0.07% [1]. However, the mortality rate from splenic abscesses remains high, especially for immunocompromised patients [2]. The best course of treatment is still unclear, but current literature demonstrates that early detection and source control have been shown to improve outcomes [2]. There are several management options available, including treatment with antibiotics, percutaneous and surgical drainage. However, surgical intervention is currently considered the standard of care due to its effectiveness compared to percutaneous drainage, which has a high inefficacy rate ranging from 14.3% to 75% [3]. Additionally, splenic abscesses pose a diagnostic challenge due to their non-specific presentation. Recent advancements in imaging modalities, such as CT scans and Ultrasonography (US), have led to higher detection rates. US, in particular, has been instrumental in detecting splenic abscesses, due to its affordability, safety, accessibility, and precision [3].
We present a unique case of a woman with end-stage renal disease on hemodialysis, who is otherwise immunocompetent presenting with septic shock from a perforated splenic abscess and pneumoperitoneum.
Case presentation
A 47-year-old female who is end-stage renal disease on hemodialysis presents to the emergency department after she was found to be hypotensive with leukocytosis at dialysis.
She denies any abdominal pain, but does have anorexia, fever, and chills. She has a history of a left ureteral stent for hydronephrosis with a nephrostomy tube that is in place. Patient states that four days ago her nephrostomy tube started showing a purulent discharge that was malodorous.
PMH: End-stage renal disease, type I diabetes mellitus, hypertension, chronic anemia, history of cerebrovascular accident requiring tPA on 10/13/2022, nonfunctional left kidney, recurrent left hydronephrosis, recurrent urinary tract infections, urinary retention, cardiomyopathy, history of MRSA bacteremia, history of diabetic ketoacidosis.
Transesophageal echocardiography: Ejection fraction 30 to 35% (10/14/2022).
PSH: Creation of AV fistula for dialysis, left nephrostomy and left ureteral stent.
Medications: Amlodipine, aspirin 81 mg, atorvastatin, calcitriol, calcium carbonate, escitalopram, ferrous sulfate, insulin aspart/detemir.
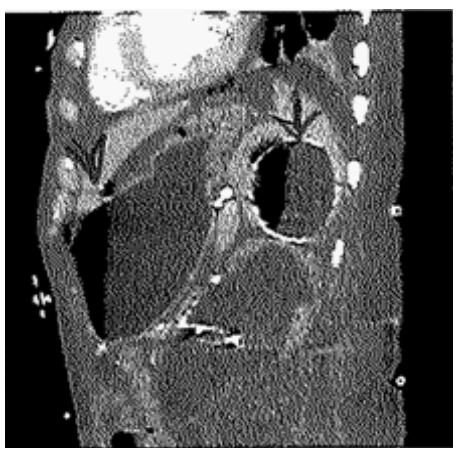
Her initial blood pressure of 74/51 mmHg was fluid responsive and blood pressure was normalized. She was noted on exam to have mild tenderness to palpation of the left upper quadrant, and she did not have rebound tenderness. She had a nephrostomy tube in the left kidney that was draining purulent fluid. She was taken to CT scan, which revealed a 6.6 cm splenic abscess with gas within capsule, pneumoperitoneum, and left sided hydronephrosis with nephrostomy tube (Figures 1 and 2).
Hemoglobin 8.3 g/L, White Blood Cells (WBC) count 20.2×109 /L with normal platelet count (247×109 /L), lactic acid was 2.2 mmol/L, and sodium was 130 mmol/L. BUN and Creatinine were both elevated, but the patient was end-stage renal disease and was undergoing dialysis.
Pneumoperitoneum and air-fluid level with air outlining the splenic cystic structure suggesting abscess.
Moderate to severe left-sided hydronephrosis.
Exploratory laparotomy, splenectomy, 19 Fr channel drain placement.
A laparotomy transverse incision was made in the left upper quadrant and the abdomen was entered in the standard fashion. Upon entry to the abdomen, it was noted that there was purulent material in the abdomen and cultures were taken. We were then able to palpate the spleen and placed lap pads in the left upper quadrant to mobilize the spleen medially, and identified the hilum of the spleen, and identified the splenic artery and vein. These structures were ligated and divided, and the spleen was removed. A 19 French channel drain was placed in the left upper quadrant. The abdomen was thoroughly irrigated. We then evaluated the retroperitoneum and found it to be completely intact with no concerns for eroding infection from the kidney. The abdomen was closed, and the patient taken to the ICU from the OR. Postoperatively, patient had uneventful recovery and was discharged to later have a left nephrectomy for unresolved chronic pyelonephritis.

Discussion
Splenic abscesses have a bimodal age distribution with peaks at 30 and 60 years of age. About two-thirds of splenic abscesses in adults are solitary, while one-third are multiple. Very rarely, a ruptured splenic abscess can cause pneumoperitoneum, and this may require the abscess to have formed secondary to a gasforming organism. Pneumoperitoneum typically occurs secondary to perforation of a hollow organ, such as gastric perforation, perforated diverticulitis/appendicitis, perforated bowel malignancy, or perforation of a strangulated intestinal obstruction. Therefore, when evaluating a patient with pneumoperitoneum, it is crucial to consider the possibility of a perforated splenic abscess in the differential diagnosis.
References
- Agarwal N, Sharma A, Garg G. BMJ Case Rep 2019; 12: e228961. doi: 10.1136/bcr-2018-228961.
- Kafadar MT, Teker İ, Gök MA, Uğurla ET, Çetinkaya İ. Atraumatic splenic rupture secondary to abscess in a hemodialysis patient: a rare and fatal cause of acute abdomen diagnosed late. J Surg Case Rep. 2018 May 22; 2018(5): rjy103. doi: 10.1093/jscr/ rjy103.
- Peña-Ros E, Méndez-Martinez M, Vicente-Ruiz M, SánchezCifuentes A, Martínez-Sanz N, et al. Neumoperitoneo por absceso esplénico: un reto diagnóstic. Reporte de un caso. Cir Cir. 2015; 83: 433-437.