
Open Journal of
Clinical and Medical Images
Case Report - Open Access, Volume 4
Unveiling osteoporosis in type 2 diabetes: A diagnostic and therapeutic challenge
Nicola Tecce1*; Fiammetta Romano1; Giulia de Alteriis1; Giovanna Muscogiuri2,3; Annamaria Colao2,3; Carla Di Somma1
1Department of Clinical Medicine and Surgery, Unit of Endocrinology, Federico II University Medical School of Naples, Via Sergio Pansini 5, 80131 Napoli, Italy.
2Department of Clinical Medicine and Surgery, Unit of Endocrinology, Italian Center for the Care and Well-being of Patients with Obesity (C.I.B.O), Federico II University Medical School of Naples, Via Sergio Pansini 5, 80131 Napoli, Italy.
3UNESCO Chair on Health Education and Sustainable Development, University Federico II, 80131 Napoli, Italy.
*Corresponding Author: Nicola Tecce
Department of Clinical Medicine and Surgery, Unit of
Endocrinology, Federico II University Medical School of
Naples, Via Sergio Pansini 5, 80131 Napoli, Italy.
Email: nicola.tecce@unina.it
Received : Feb 20, 2024
Accepted : Mar 14, 2024
Published : Mar 21, 2024
Archived : www.jclinmedimages.org
Copyright : © Tecce N (2024).
Abstract
This case report explores the complex relationship between Type 2 Diabetes Mellitus (T2DM) and osteoporosis, highlighting the diagnostic and therapeutic challenges encountered. It presents the journey of P.M, a 55-year-old woman with a 10-year history of T2DM, who was initially screened for osteopenia with MOC DEXA, which failed to accurately diagnose her condition. Subsequent dorsolumbar radiography revealed significant osteoporosis, leading to an integrated treatment approach with denosumab, lifestyle changes, and careful diabetes management. The case highlights the limitations of traditional diagnostic methods in diabetic patients and underscores the need for personalized, comprehensive care strategies to address both diabetes and osteoporosis, illustrating the potential for improved outcomes through targeted therapies and ongoing patient monitoring. This report contributes to a broader understanding of the management of complex comorbid conditions and underscores the need for continued innovation in clinical practice.
Keywords: Osteoporosis; Type 2 diabetes mellitus; DEXA; Dorsolumbar RX; Denosumab.
Citation: Tecce N, Romano F, Alteriis GD, Muscogiuri G, Colao A, et al. Unveiling osteoporosis in type 2 diabetes: A diagnostic and therapeutic challenge. Open J Clin Med Images. 2024; 4(1): 1174.
Introduction
Osteoporosis has been for a long time considered a systemic skeletal illness caused by low bone mass, leading to an increase in fragility fracture risk. It is nowadays well known that alterations in bone quality and the micro-architectural degeneration of bone tissue also have a great counterpart in the development of the fragility that marks this disease, beyond the Bone Mineral Density (BMD) itself [1]. A perfect example of this is the complex relationship between Type 2 Diabetes Mellitus (T2DM) and osteoporosis, which underscores the paradox in which individuals with T2DM often have increased BMD yet are at increased risk of fracture. This suggests that factors other than BMD contribute to increased bone fragility in this population. The pathogenesis of osteoporosis in T2DM involves a complex interplay of metabolic abnormalities. Despite the anabolic effects of insulin on bone, the insulin resistance and hyperinsulinemia characteristic of T2DM indirectly affect bone quality, leading to an increased risk of fracture [2]. Advanced Glycation End Products (AGEs) resulting from prolonged hyperglycemia affect bone quality by altering the collagen matrix and reducing bone strength, contributing significantly to the osteoporotic process in diabetes [3]. The role of inflammatory cytokines and adipocytes, which are elevated in T2DM due to obesity and metabolic dysregulation, further complicates the relationship between diabetes and bone health by affecting bone turnover and bone quality. Osteoblast dysfunction in the diabetic milieu impairs bone formation and remodeling, which is central to the development of osteoporosis in T2DM patients [4]. From a healthcare perspective, the unique bone disease profile in T2DM - characterized by increased BMD but higher fracture risk - poses significant challenges for the diagnosis, prevention, and treatment of osteoporosis in these patients. This calls for an integrated approach within healthcare systems that focuses on both diabetes management and proactive assessment and treatment of bone health. Innovative screening and monitoring strategies are needed to accurately assess fracture risk beyond traditional BMD measurements. Prevention and treatment strategies for osteoporosis in T2DM must address lifestyle factors, optimize glycemic control, and consider the impact of antidiabetic medications on bone health. Educating patients about the importance of bone health and fracture prevention strategies is critical to managing the dual burden of T2DM and osteoporosis. As the prevalence of T2DM continues to rise, a better understanding of its association with osteoporosis and the development of effective management strategies are key to reducing fracture risk and improving patient outcomes.
Case presentation
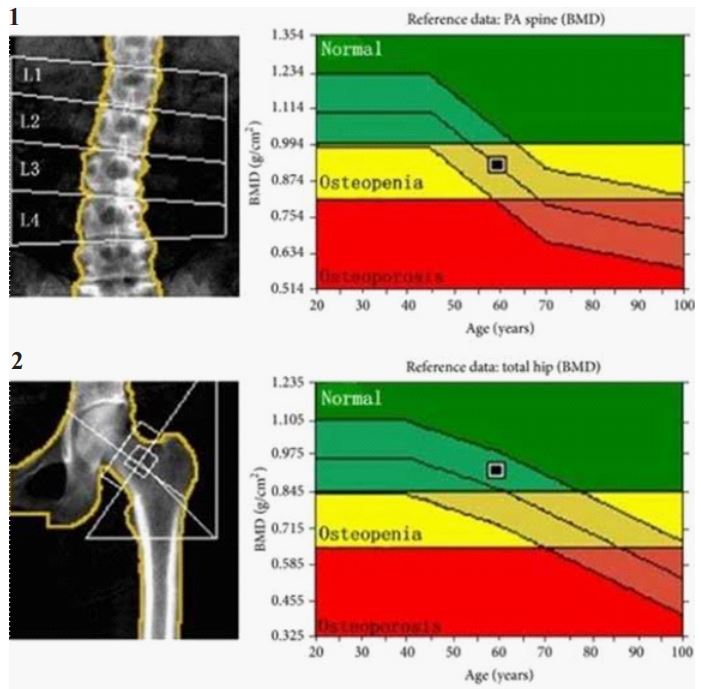
P.M., a 55-year-old woman, came to our clinic without a prior diagnosis of osteoporosis, despite a family history of the condition. Regular in her bowel and urinary habits, she reached menarche at 12 and menopause at 53, with a history of one spontaneous abortion. A heavy smoker, consuming 50 cigarettes daily, her diet is calorically dense yet lacks adequate calcium-she avoids milk, dairy, and calcium-fortified water. Her medical history is significant for GERD, arterial hypertension, mixed dyslipidemia, and type 2 diabetes mellitus, which she has managed for ten years with dulaglutide and metformin, maintaining reasonable glycemic control. A sedentary lifestyle, a waist circumference of 96 cm, and lab values indicative of metabolic syndrome augment her fracture risk, compounded by postmenopausal osteoporosis and the deleterious effects of smoking on bone density. Her medical journey began when routine MOC (Measurement of Cortical Bone) DEXA scans, initially suggestive of osteopenia, prompted a closer examination due to her decade-long battle with type 2 diabetes. MOC DEXA is a specialized form of Dual-Energy X-Ray Absorptiometry (DEXA) that focuses on cortical bone density and is commonly used to assess bone health and diagnose osteoporosis. It provides accurate measurements of Bone Mineral Density (BMD), which is critical for assessing fracture risk. Recognizing the limitations of MOC DEXA in accurately diagnosing osteoporosis in diabetic patients - where false negatives can occur due to altered bone quality - our team decided to assess the patient’s individual fracture risk using two different algorithms: FRAX and DeFRA. The FRAX score is an assessment tool that estimates a patient’s 10-year fracture risk based on several factors, including age, gender, weight, previous fractures, and smoking status, among others. DEFRA is a derivative tool designed for more specific populations or conditions that enhances fracture risk assessment by incorporating additional clinical factors to provide a tailored risk assessment. These tools can guide clinical decisions regarding the need for treatment or further diagnostic evaluation in the management of osteoporosis. However, the fracture risk at 10 years calculated for our patients did not result to be significatively high with both the algorithms (DeFra score: 5.3%; Frax score for major osteoporotic fractures: 8.6%; Frax score for hip fracture: 0.1%). At this point we could have finished our diagnostic process. Nevertheless, taking into account the patient’s long history of diabetes, high tobacco consumption and family history of osteoporosis, as well as the finding on clinical examination of a height reduced by 4 cm compared to that reported at the age of 25 years, we opted for a more comprehensive diagnostic approach with subsequent dorsolumbar RX. Dorsolumbar RX (radiography) is a traditional imaging technique that captures detailed images of the dorsal and lumbar regions of the spine. It’s used in the diagnosis of osteoporosis to visually identify vertebral fractures, deformities, or significant bone loss that may not be detected by DEXA scans alone. The dorsolumbar RX revealed the true extent of her condition: significant osteoporosis hidden beneath the surface of standard screening methods. Two vertebral fragility fractures (I and III grade) and less significant vertebral deformities, measured with the Genant semi quantitative method, were found. Genant method is a visual grading system for vertebral fractures detected on a lateral spinal radiograph [5]. This revelation was a turning point in P.M.’s care. Because diabetes complicates her osteoporosis treatment, we carefully considered her management plan. Diabetes, especially long-term diabetes, can affect bone quality and healing, requiring a nuanced approach to treatment. Denosumab, chosen for its efficacy in increasing bone density and reducing fracture risk in patients with diabetes, marked the beginning of her targeted osteoporosis therapy. This biannual injection, along with vitamin D supplementation, tight glycemic control and lifestyle changes, was designed to reduce her fracture risk while managing her diabetes. The decision to start denosumab was based not only on its proven benefits for bone health, but also on its compatibility with diabetic patients, who face unique challenges in bone metabolism and healing. P.M.’s treatment was complemented by a rigorous follow-up program, monitoring for potential side effects of the therapy, and adjustments to her diabetes management to ensure optimal care.
Management and outcome
With the revelation of significant osteoporosis via dorsolumbar RX, as opposed to the initial MOC DEXA findings of simple osteopenia, the patient’s management strategy required careful planning. Given the complicating factor of a 10-year history of type 2 diabetes, the treatment approach had to consider both the immediate needs of bone health and the overarching influence of diabetes management. Denosumab was selected for its dual benefit of improving bone density and its suitability for patients with diabetes, which is known to adversely affect bone metabolism. The initiation of denosumab, coupled with vigilant diabetes control and lifestyle interventions, aimed to comprehensively treat the patient’s osteoporosis while mitigating any diabetes-related deterioration in bone health. This holistic management plan underscored the importance of personalized care tailored to the multifaceted needs of patients with complex comorbidities. The results of this integrated approach were promising. Over the course of treatment, the patient showed improvements in bone density metrics measured at subsequent follow-up visits, along with stable glycemic levels. This positive trend not only demonstrated the efficacy of denosumab in this patient’s context, but also highlighted the critical role of a coordinated treatment strategy that addresses both osteoporosis and diabetes management. The case illustrates the potential for significant patient outcomes through the judicious use of targeted therapies and underscores the need for ongoing monitoring and adjustment of treatment protocols to best meet individual patient needs.
The dorsolumbar RX revealed the true extent of her condition: significant osteoporosis hidden beneath the surface of standard screening methods. Two vertebral fragility fractures (I and III grade) and less significant vertebral deformities, measured with the Genant semi quantitative method, were found.
Discussion
This case highlights the limitations of traditional diagnostic modalities such as MOC DEXA in patients with diabetes, where bone quality may be disproportionately affected, leading to potentially misleading assessments. The successful use of dorsolumbar RX to reveal significant osteoporosis where MOC DEXA showed only osteopenia underscores the need for a more nuanced diagnostic approach in diabetic patients. In addition, this case highlights the importance of an integrated management strategy that not only addresses osteoporosis with treatments such as denosumab, but also carefully manages diabetes, which can significantly impact bone health. The favorable outcome achieved in this patient, with improved bone density and stable glycemic control, demonstrates the potential benefits of such a tailored approach. The broader implications of this case for clinical practice include the need for increased awareness of the complex interactions between diabetes and bone health, advocating for a more comprehensive evaluation of osteoporosis in diabetic patients. It also calls for ongoing research to optimize diagnostic and treatment strategies for this patient population, ensuring that care is both effective and individualized.
Conclusion
This case highlights the need for comprehensive diagnostic strategies beyond standard practices to uncover the true extent of osteoporosis in patients with diabetes. It also demonstrates the effectiveness of tailored treatment plans, such as the use of denosumab in conjunction with diabetes management, in improving patient outcomes. This report contributes to the evolving understanding of the management of complex comorbid conditions and highlights the need for continued research and innovation in clinical practice to improve patient care.
Declarations
Patient consent: Consent was obtained from the patient to share her case details.
Declaration of conflicting interests: We, the authors, declare that we have no conflict of interest regarding this manuscript. We did not receive any funding or support from any organization or entity that would have a financial interest in the publication of this manuscript. Additionally, we have no financial relationships with any companies or organizations that might have a direct or indirect interest in the content of this manuscript. Therefore, there is no conflict of interest to disclose.
References
- Commissione Intersocietaria per l’Osteoporosi (SIE, SIGG, SIMFER, SIMG, SIMI, SIOMMMS, SIR, SIOT)]. Linee Guida sulla gestione dell’Osteoporosi e delle Fratture da fragilità. 2021.
- Sealand R, C Razavi, RA Adler, Diabetes Mellitus and Osteoporosis. Current Diabetes Reports. 2013; 13(3): 411-418.
- Akin O, et al. Evaluation of bone turnover in postmenopausal patients with type 2 diabetes mellitus using biochemical markers and bone mineral density measurements. Gynecological Endocrinology. 2003; 17(1): 19-29.
- Viégas M, et al. Prevalence of osteoporosis and vertebral fractures in postmenopausal women with type 2 diabetes mellitus and their relationship with duration of the disease and chronic complications. J Diabetes Complications. 2011; 25(4): 216-21.
- Genant HK. Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semi quantitative technique. J Bone Miner Res. 1993; 8(9): 1137-48.