
Open Journal of
Clinical and Medical Images
Short Report - Open Access, Volume 4
Acorn Traser dual mobility cup: Osseo Integration signs
Domenico Tigani*; M Cuzzani; L Solito; C Donadono; G Pieratelli; L Banci; G Melucci
Department of Orthopedic Surgery, Ospedale Maggiore C.A. Pizzardi, Largo B. Nigrisoli 2, 40133, Bologna, Italy.
*Corresponding Author: Domenico Tigani
Department of Orthopedic Surgery, Ospedale Maggiore
C.A. Pizzardi, Largo B. Nigrisoli 2, 40133, Bologna, Italy.
Email: domenico.tigani@ausl.bologna.it
Received : Feb 21, 2024
Accepted : Mar 15, 2024
Published : Mar 22, 2024
Archived : www.jclinmedimages.org
Copyright : © Tigani D (2024).
Abstract
Keywords: Total hip arthroplasty; Dual Mobility Cup; 3Dprinted highly-porous titanium.
Citation: Tigani D, Cuzzani M, Solito L, Donadono C, Pieratelli G, et al. Acorn Traser dual mobility cup: Osseo Integration signs. Open J Clin Med Images. 2024; 4(1): 1175.
Introduction
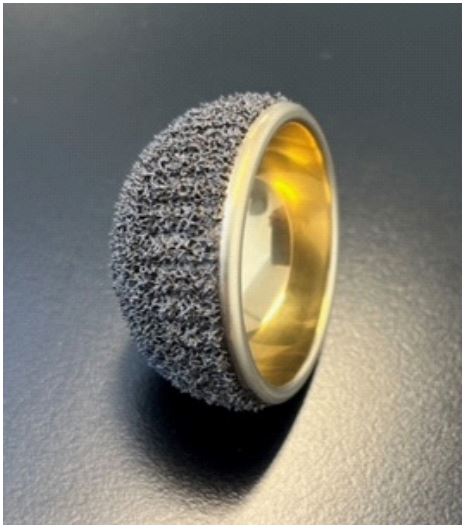
The use of 3D-printed highly porous titanium acetabular cups is becoming popular in Total Hip Arthroplasty (THA) [1,2]. Their porosity mimics that of natural cancellous bone, leading to hopes for more rapid and effective osseo integration compared to traditional titanium and HA-coated implants [1,2]. The Acorn Traser cup (Permedica Orthopaedics S.p.A., Merate, Italy) is a new cement less monobloc Dual Mobility Cup (DMC) recently introduced to the market [3,4]. The cup features a highly porous trabecular structure (Traser) on the bone-cup surface and a titanium-niobium nitride (TiNbN) ceramic coating on the articular side to improve tribological behavior of the titanium shell against the mobile liner. Traser has 70% permeable porosity with a mean pore size of 520 μm. The rationale for using a Ti alloy highly porous DMC is manifold: to prevent any possible adverse reactions due to corrosion of CoCrMo and stainless steel implants, which have been the standard materials for currently available DMC shells. With The Introduction of an Inner Titanium-Niobium Nitride (TiNbN) ceramic coating surface, it was possible to overcome the poor tribological quality of titanium. Another interesting characteristic is the higher implant radiolucency that might facilitate radiographic assessment of cup orientation, even in anterior-posterior projection, and allow for the calculation of cup ante version and measurement of polyethylene wear, which are crucial in studying the durability of THA.
The aim of this paper is to radiographically determine the presence of the different signs of Osseo integration described by Moore et al., which are predictors of implant stability, using this new DMC implant. Particularly, we seek:
Absence of radiolucent lines;
Presence of a superolateral buttress;
Medial stress-shielding;
Radial trabeculae; and
An inferomedial buttress (Figure 1).
The Acorn Traser cup, characterized by highly porous trabecular structure (70% permeable porosity with a mean pore size of 520 μm) on the external surface and a TiNbN ceramic coating on the articular side (Image courtesy of Pdermedica Orthopedics).


Conclusion
The evolution of DMCs has progressed through several steps over a long period of almost fifty years, culminating in the development of highly porous cup surfaces, which represent a significant design change from past DMC generations. This new material could mark the beginning of a new generation of highly porous implants, even in the field of DMCs. However, these changes must be accompanied by rigorous evaluations of clinical outcomes as well as genuine improvements in osteointegration capacity. Titanium and titanium alloy cups with highly porous surfaces have been developed relatively recently for traditional prostheses. Due to differences in materials, production processes, and porosity, the promising success of some implants [1,2,4] should not be generalized to all third-generation titanium cups [5-7].
Valid signs of bony ingrowth have been observed during the first 12 months of follow-up in all our cases, with no signs of radiolucency. In the latest follow-up, we found a prevalence of superolateral buttress and medial stress-shielding, with radial trabeculae and inferomedial buttress occasionally observed. In cases where gaps were present (areas without initial bonecup contact in the immediate post-operative X-rays), they were completely filled within the first three months post-operatively. No cup or liner revisions were performed, and no cases of radiographic loosening were observed in the latest follow-up.
In the last follow-up, we primarily observed the presence of superolateral buttress and medial stress-shielding, with radial trabeculae and inferomedial buttress occasionally present (Figure 2).
Plain radiograph of a highly porous titanium dual mobility cup implant used in primary Total Hip Arthroplasty (THA) for hip secondary osteoarthritis.
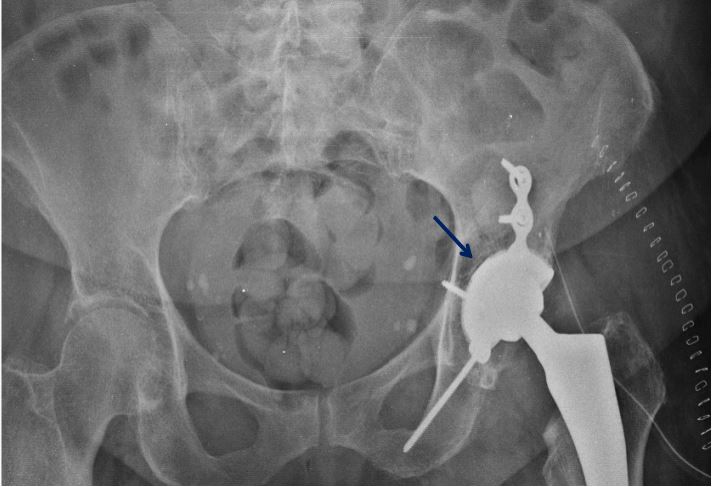
Post-operative radiograph of the pelvis with both hips in an anteroposterior view showing post-traumatic arthritis in the left hip following fixation for acetabular fractures.
Post-operative radiograph following total hip arthroplasty performed with the Acorn Traser® DM cup, without the need for plate and screw removal. A small gap area is observed in DeLee and Charnley Zone II (Blue arrow).
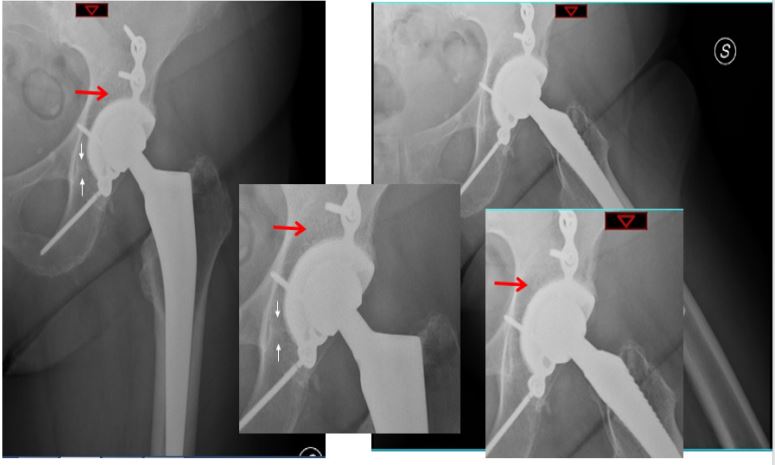
Anterior-posterior and lateral (D) radiographs at the 12-month follow-up after total hip arthroplasty, showing complete filling of the gap and the presence of radial trabeculae perpendicular to the surface of the cup in DeLee and Charnley Zone I or Zone II (red arrows and close-up images).
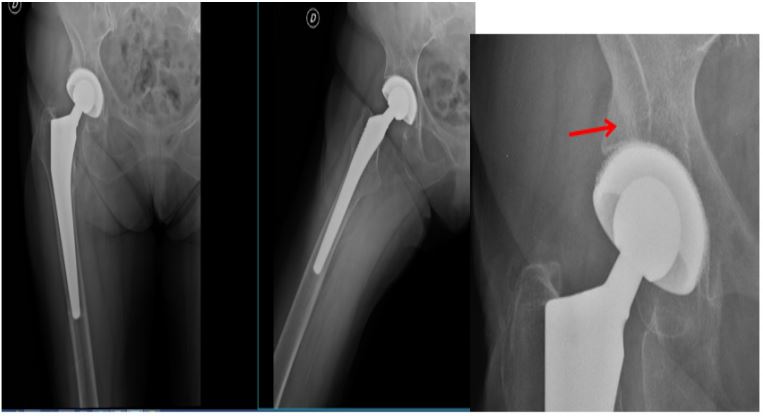
AP X-ray of the pelvis showing a femoral neck fracture of the right hip (A).
12-month radiograph after total hip arthroplasty performed with the Acorn Traser® DM cup, demonstrating the presence of superolateral buttresses (B).
References
- Commissione Intersocietaria per l’Osteoporosi (SIE, SIGG, SIMFER, SIMG, SIMI, SIOMMMS, SIR, SIOT)]. Linee Guida sulla gestione dell’Osteoporosi e delle Fratture da fragilità. 2021.
- Sealand R, C Razavi, RA Adler, Diabetes Mellitus and Osteoporosis. Current Diabetes Reports. 2013; 13(3): 411-418.
- Akin O, et al. Evaluation of bone turnover in postmenopausal patients with type 2 diabetes mellitus using biochemical markers and bone mineral density measurements. Gynecological Endocrinology. 2003; 17(1): 19-29.
- Viégas M, et al. Prevalence of osteoporosis and vertebral fractures in postmenopausal women with type 2 diabetes mellitus and their relationship with duration of the disease and chronic complications. J Diabetes Complications. 2011; 25(4): 216-21.
- Genant HK. Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semi quantitative technique. J Bone Miner Res. 1993; 8(9): 1137-48.