
Open Journal of
Clinical and Medical Images
Case Series - Open Access, Volume 4
Premixed hyaluronic acid and calcium hydroxyapatite dermal fillers: A new generation of aesthetic injectables case presentation and review of literature
Marko Mance1,2*; Elvira Lazić Mosler2,3,4
1University Hospital Centre Zagreb, Croatia.
2Private Clinic, Skin Health Lab, Zagreb, Croatia.
3Catholic University of Croatia, School of Medicine, Zagreb, Croatia.
4Department of Dermatology, General Hospital “Dr Ivo Pedišić Sisak”, Sisak, Croatia.
*Corresponding Author: Marko Mance
University Hospital Center Zagreb, Croatia.
Email: markomance@gmail.com
Received : Feb 23, 2024
Accepted : Mar 26, 2024
Published : Mar 29, 2024
Archived : www.jclinmedimages.org
Copyright : © Mance M (2024).
Abstract
Dermal fillers based on hyaluronic acid, despite being on the market for almost 30 years, remain unflaggingly popular among both doctors and patients. This happens because hyaluronic acid dermal fillers are safe, long-lasting, non-immunogenic, available to most patients, and can be removed with hyaluronidase. The use of fillers based on hyaluronic acid in correcting deficits in the upper, mid and lower part of the face, can significantly improve the balance and appearance of the face. Below we present two patients who underwent dermal filler facial injections due to their dissatisfaction with their aging appearance. They were given a questionnaire - PESRT (Patient Evaluation of Skin Rejuvenation Treatments) developed in our clinic before and 6 weeks after treatment to grade their opinions and results using a percentage scale. This case report demonstrated that hyaluronic acid filler cross linked with poly (ethylene glycol) diglycidyl ether was effective and well tolerated for volume augmentation. The subjects were very satisfied with her experience of the hydrogel and natural-looking results were achieved.
Keywords: Hyaluronic acid; Calcium hydroxyapatite; Dermal fillers; Cross-linking; PEG.
Abbreviations: HA: Hyaluronic Acid; PEG: Poly Ethylene Glycol; PEGDE: Poly (Ethylene Glycol) Diglycidyl Ether; BDDE: Butanediol Diglycidyl Ether.
Citation: Mance M, Mosler EL. Premixed hyaluronic acid and calcium hydroxyapatite dermal fillers: A new generation of aesthetic injectables case presentation and review of literature. Open J Clin Med Images. 2024; 4(1): 1178.
Introduction
Facial aging is a multifactorial process governed by a multitude of external and internal factors. It occurs as a complex three-dimensional process affecting different anatomical layers including muscle, bone, adipose tissue and cutaneous changes including loss of elasticity and thinning of the skin layers [1]. As an individual ages, there is a marked decrease in dermal thickness and reduced production of collagen attributing to not only a substantial loss of volume, but skin quality as well.
With the popularization of minimally invasive aesthetic treatments injectable facial fillers have revolutionized our ability to restore volume loss and rejuvenate of the aging face [2]. This has also led to a better understanding of the science of aging and the subsequent development of more advanced products catering to the growing demand for better results and safer treatments. Currently both Hyaluronic Acid (HA) and Calcium Hydroxyapatite (CaHA) based fillers top the ranking list of nonsurgical aesthetic procedures worldwide [3]. These products have their defined specific treatment targets, with HA being used for more for volumization while CaHA is traditionally used more as a biostimulator for collagen synthesis stimulation [3,4].
The effect of HA dermal fillers is mainly based on strategic deposition of filler in the different facial tissue layers and compartments leading to a volumizing effect. Due to its compressible nature, HA dermal fillers are considered ideal in areas where bone structures are well-defined or where the skin is thin [5].
HA dermal fillers used in aesthetic medicine are characterized as viscoelastic, measured by the complex modulus, which is the sum of the elastic modulus (G′) with the viscous modulus (G″). The elastic modulus (G′) is regarded as the firmness of the gel and measures the resistance of a material to deformation. This is best understood as the stiffer the material then the higher the G′ [6]. This characteristic is determined by the degree and strength of the HA cross-linking properties as well as the HA concentration. Clinically, this becomes important since gels with a higher G′ will have better resistance to the dynamic forces caused by muscle movement; which is ideal for areas such as the nasolabial folds and marionette lines. In contrast, areas with more superficial wrinkles or static skin changes, resistance to deformation by muscle movement is less critical and gels with lower G′ are a better treatment choice. These gels are also better suited for areas that require a softer feel, such as the lips. G” is the viscous modulus of the energy fraction that is lost under shear deformation. G” reflects the inability of the gel to recover its original shape after a shear force is removed. Clinically, G” is related to inject ability [2].
CaHA is a natural substance regularly found in humans and its synthetic microspheres are biocompatible and biodegradable offering a high safety profile as an injectable. Histologically, these particles induce a histiocytic and fibroblastic tissue response in the dermis, leading to increased collagen formation and subsequent indirect volumization, tissue-lifting and skintightening [6]. In some instances, it has been shown that CaHA can have a stronger skin tightening and tissue lifting effect compared to HA only treatment [7].
The synergistic effect of both HA and CaHA has been recognized by most aesthetic physicians and it is known that HA and CaHA compounds can be applied in the same treatment area, resulting in better outcomes compared with only one individual treatment [1]. These outcomes have led to the development of dermal fillers with premixed HA and CaHA. Although the rheological properties are changed with this combination, great results with an acceptable safety profile have been reported with this technique [3,8,9]. It is important for the physician to understand the biophysical properties of this new generation of dermal fillers, as these constitute the clinical outcomes and safety profile of the product.
Case presentation
We present two patients who underwent dermal filler facial injections due to their dissatisfaction with their aging appearance. They were given a questionnaire - PESRT (Patient Evaluation of Skin Rejuvenation Treatments) developed in our clinic before and 6 weeks after treatment to grade their opinions and results using a percentage scale. The dermal fillers used were all using the Neauvia hydrogels line (MatexLab, Geneva, Switzerland) and included: Neauvia Intense (28 mg/ml HA, glycine and L-proline), Neauvia Stimulate (26 mg/ml HA, calcium hydroxyapatite (1%), glycine and L-proline), Neauvia Intense Lips (24 mg/ml HA, glycine and L-proline) and Neauvia Hydro Deluxe (non-cross-linked HA 18 mg/ml, calcium hydroxyapatite 0.01%, glycine, and l-proline).
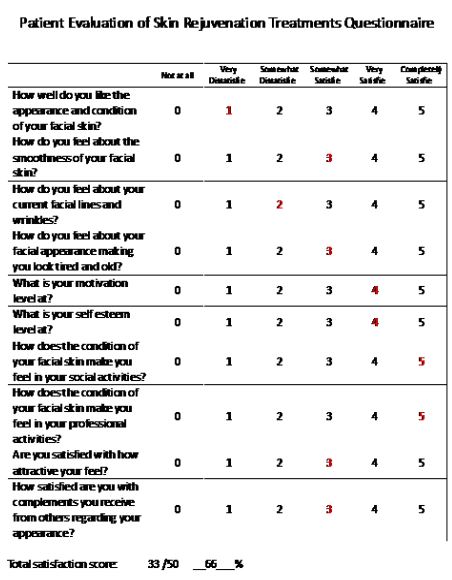
Patient 1: 36 year old female patient who presented with dissatisfaction of her drooping malar regions, lack of jaw definition and poor skin quality. She scored 66% on her PESRT questionnaire before treatment (Figure 1).
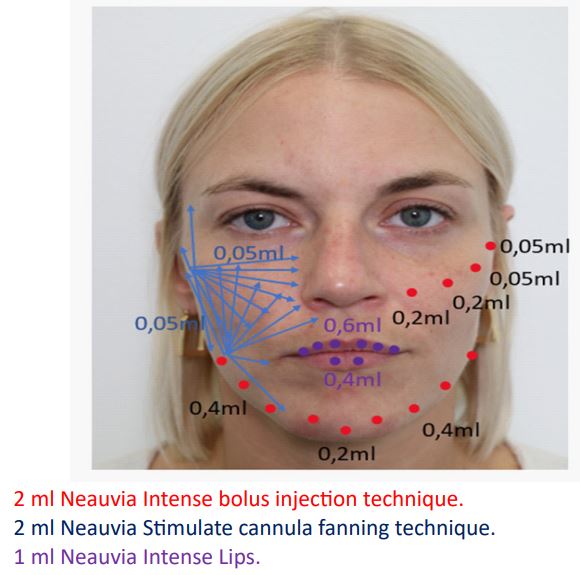
She was treated with 2 ml Neauvia Intense dermal filler using the needle-bolus technique to her malar and mandibular regions for deep volume restoration. 2 ml Neauvia Stimulate to her midface and temporal regions using cannula for contouring definition and skin quality enhancement and 1 ml Neauvia Intense Lips for lip definition (Figure 2).

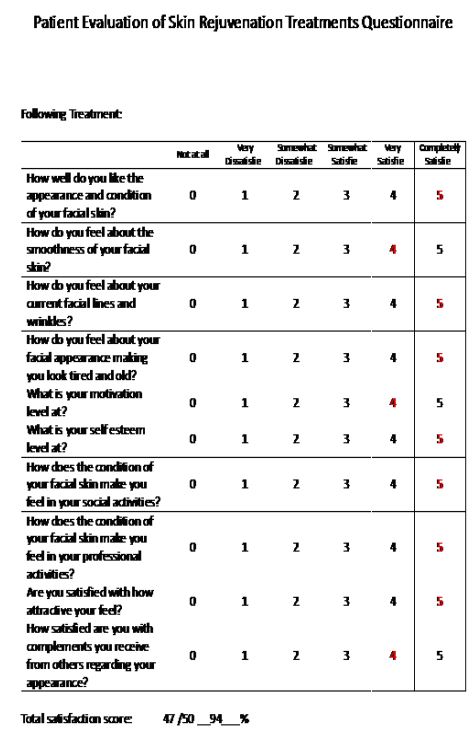
6 weeks following treatment she was evaluated. She had visually marked volumization and improvement in her malar and jaw line regions. Her lips were more pronounced and fuller. She had marked improvement in her skin tone and smoothness, with less rosacea and colour blemishes (Figure 3). She was asked to fill out her PESRT questionnaire which showed improvements in all aspects, particularly regarding skin quality, smoothness, fine lines and wrinkles. 6 weeks following treatment her PESRT score was 94%, showing a 28% improvement (Figure 4).
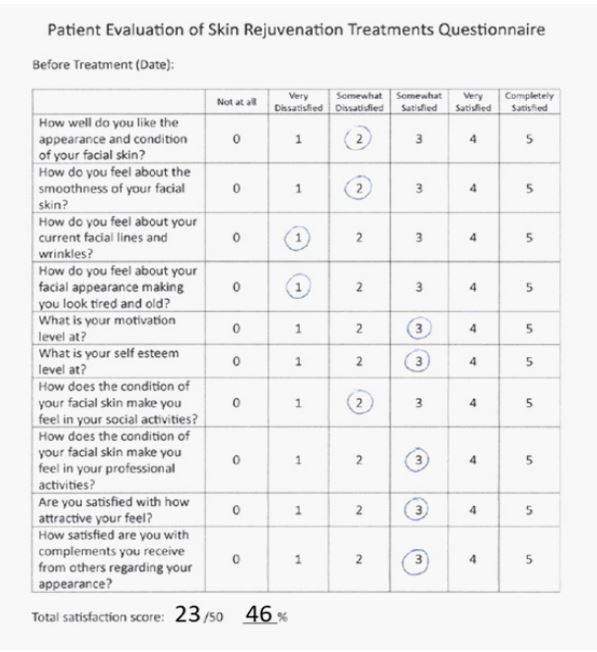
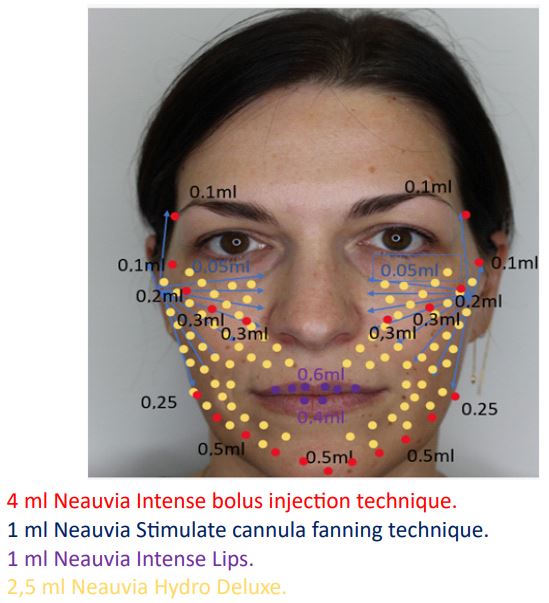
Patient 2: 39 year old female patient who presented with dissatisfaction of her depressed appearance in the malar regions, skin laxity, nasolabial fold crease, dry and poor skin quality and overall tired appearance. She scored 46% on her PESRT questionnaire before treatment (Figure 5). On all of the presented questions, there was not one aspect of her appearance that she considered very or completely satisfied.
She was treated with 4 ml Neauvia Intense dermal filler using the needle-bolus technique to her malar, mandibular and temporal regions for deep volume restoration. 1 ml Neauvia Stimulate to her midface and temporal regions using cannula for contouring definition and skin quality enhancement, 2.5 ml Neauvia Hydro Deluxe for mid and lower face rehydration and 1 ml Neauvia Intense Lips for lip enhancement (Figure 6).

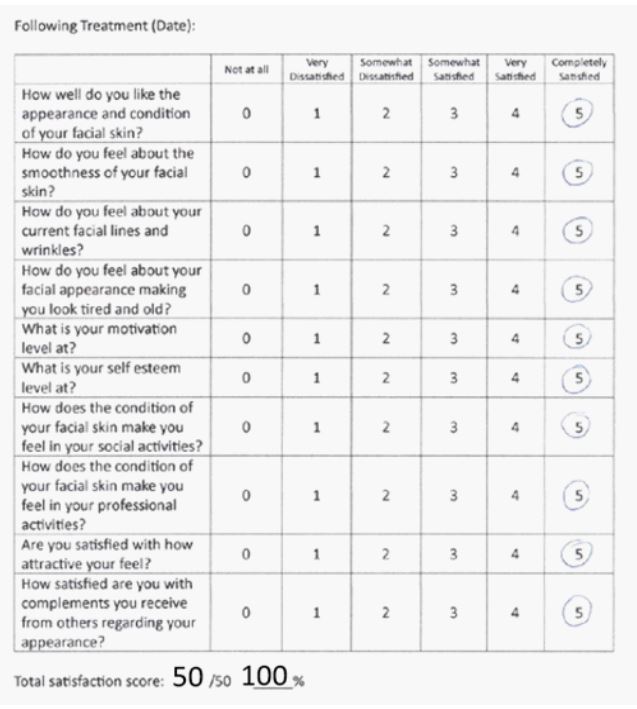
6 weeks following treatment she was evaluated. She had visually marked volumization and improvement in her malar and temporal regions. Her lips were also more pronounced and fuller. She had marked improvement in her skin tone, facial contours and smoothness, with less fine line wrinkles and less definition of her nasolabial fold crease (Figure 7). She was asked to fill out her PESRT questionnaire which showed improvements and complete satisfaction in all aspects, particularly regarding skin condition, appearance and self-esteem. 6 weeks following treatment her PESRT score was 100%, showing a 54% improvement (Figure 8).
Discussion
The use of facial fillers for aesthetics treatments is not a new concept. Origins trace back to the 19th century when the German physician, Dr. Franz Neuber used autologous fat as a soft tissue filler for cosmetic deformity [10]. Until the early 1980s, none of the previously attempted facial fillers that were silicone or teflon based had received FDA approval until the bovine collagen, Zyderm (Inamed Corp., Santa Barbara, CA) was approved in 1981. Even with an increase in research, bovine collagen was the only FDA approved filler for the next two decades until 2003 when the FDA approved the first HA dermal filler (Restylane; Galderma, Ft. Worth, TX). Since this approval, there has been a dramatic increase in the number of FDA approved facial fillers in response to the growing popularity of minimally invasive facial rejuvenation procedures [2].
ArteFill (Suneva Medical, San Diego, CA) is a Poly Methyl Meth Acrylate (PMMA) and collagen filler that was first developed over 20 years ago in Germany as Arteplast and its second generation successor, Artecoll. Although both fillers had adequate soft tissue filler capabilities, they also had an unacceptable rate of granuloma formation and were not approved by the FDA [2].
Polylactic acids were originally synthesized by French chemists in 1954 from the α-hydroxy-acid family. It was approved by the FDA in 2004 for soft tissue restoration in lipoatrophy in HIV patients, this was later expanded to include cosmetic applications in 2009 as Sculptra (Dermik Laboratories, Berwyn, PA) [2].
Radiesse (Merz North America, Greensboro, NC) is a synthetic, semisolid filler composed of 30% calcium hydroxyapatite and 70% carrier gel that was initially approved in 2006 for the treatment of facial wrinkles and folds as well as HIV-associated facial atrophy and then later approved in 2009 for more cosmetic applications [2].
Over the past 2 decades we have seen a vast amount of products of different chemical composition offered on the aesthetic market. The most popular dermal fillers used today are based on HA which is a glycosaminoglycan composed of Dglucuronic acid and N-acetyl-D-glucosamine naturally found in the dermis. At physiologic pH, it has excellent biocompatibility, as it is anionic, binding water extensively where 1 g of HA can bind up to 6 L water [2]. To be utilized as a soft tissue filler, the natural rapid solubility of HA needed to be chemically modified at the carboxyl acid group, and cross-linking with dialdehydes and disulfides was necessary to change its mechanical properties. This modification increases gel firmness and half-life of the product [2]. It is important to recognize that the different compositions of the chemically modified HA fillers are specific to each manufacturer and these differences create variations in quality, duration of action and safety profile amongst the HA products available. The concentration of HA in each product also varies with each manufacturer and is typically listed as the total amount of HA (soluble and insoluble HA, mg/mL) [11]. Subcutaneous swelling among different products and manufacturers varies and can partially be attributed to the molecular characteristic of HA, the concentration, amount of cross-linking, and the products used to hydrate the gel [11].
Over the past 2 decades we have seen a vast amount of products of different chemical composition offered on the aesthetic market. The most popular dermal fillers used today are based on HA which is a glycosaminoglycan composed of Dglucuronic acid and N-acetyl-D-glucosamine naturally found in the dermis. At physiologic pH, it has excellent biocompatibility, as it is anionic, binding water extensively where 1 g of HA can bind up to 6 L water [2]. To be utilized as a soft tissue filler, the natural rapid solubility of HA needed to be chemically modified at the carboxyl acid group, and cross-linking with dialdehydes and disulfides was necessary to change its mechanical properties. This modification increases gel firmness and half-life of the product [2]. It is important to recognize that the different compositions of the chemically modified HA fillers are specific to each manufacturer and these differences create variations in quality, duration of action and safety profile amongst the HA products available. The concentration of HA in each product also varies with each manufacturer and is typically listed as the total amount of HA (soluble and insoluble HA, mg/mL) [11]. Subcutaneous swelling among different products and manufacturers varies and can partially be attributed to the molecular characteristic of HA, the concentration, amount of cross-linking, and the products used to hydrate the gel [11].
Furthermore, with the natural evolution of aesthetic medicine driven by the increasing demand for less invasive procedures, we have seen an adaptation to the opinion that skin quality and tissue regeneration is almost always required in conjunction with volume replacement. With hyaluronic acid-based injectable fillers currently the golden standard for volumization procedures and calcium hydroxyapatite the second most used facial filler, it was only natural that we see dermal fillers that consist of both these substances developed [8].
Fakih-Gomez N. and Kadouch J. in their paper observed the benefits of HA and CaHA combined dermal fillers. They stated how CaHA has a stronger tissue-lifting and skin-tightening effect compared to HA fillers alone. They observed how premixing HA with CaHA can add neocollagenesis properties to a HA filler, whereas a high G’ HA dermal filler can enhance the CaHA mechanism of action by adding additional volumization while securing tissue softness. They also note how the HA can compensate for early volume loss associated with CaHA-treated areas due to rapid absorption of the carboxymethylcellulose gel carrier before the CaHA particle-induced neocollagenesis has taken effect. Also, CaHA is known to have a longer effect than most HA fillers and therefore, premixing CaHA with HA can prolong the effect of the filler treatment while improving skin quality [8,12].
Corduff N. introduced the concept of Aesthetic Regenerative Scaffolds (ARS). It is based on the known concepts that aging reduces fibroblast number and function leading to a downregulation of extracellular matrix genes and subsequent dermal thinning, solar elastosis, impaired or reduced elastin and collagen concentrations, with less tensile skin. His ARS concept focuses on the opinion that injectable biomaterials can be used to divert the fibrotic foreign body responses and subsequent fibrotic changes commonly associated with the aging process and shift the homeostatic process towards tissue regeneration; mainly ECM elements including collagen, elastin, MMPs, and glycoproteins like fibronectin, and laminins [13].
One molecule that has been associated as an aesthetic regenerative scaffold by Corduff N. is CaHA [13]. A dermal filler that uses a combination of CaHA incorporated in a HA gel is Neauvia Stimulate (Matex Lab, Geneva, Switzerland). For aesthetic purposes, the use of CaHA microspheres provides a non-permanent volumizing effect and generates ECM tissue support. CaHA also plays an important role in the rheological profile of the HAbased dermal filler as it provides a higher elastic modulus (G’) and viscosity (η) than HA only fillers 1 [4]. This HA based filler is a cross-linked monophasic polymeric hydrogel, containing stabilized sodium hyaluronate 26 mg/mL and calcium hydroxyapatite (1%), glycine and L-proline in buffer pyrogen-free water, with a modification degree range of 6.2% and with an effective crosslinker ratio of 0.07 [15]. Neauvia hydrogels are unique as they are based on PEGDE (polyethylene glycol diglycidyl ether) cross-linking technology which appears to have increased biocompatibility, excellent bio integration, and optimal rheological characteristics [16,17]. Neauvia hydrogels crosslinked with PEG (N-Gel) have a very high safety profile and low toxicity value that is considered lower than other cross-linking agents commonly used [13,18]. This is due to the fact that N-Gel has shown to modulate critical functions of human Poly Morph Nuclear Neutrophils (PMN) such as migration and oxidative metabolism. The non-toxicity and non-immunogenicity characteristics of PEG results in an anti-inflammatory outcome that minimizes the potential for allergic and immunological reactions [16,19].
When comparing PEG with the most frequently used HA based dermal filler crosslinking molecule 1,4-Butanediol Diglycidyl Ether (BDDE), their properties differ to a large degree. As a crosslinking agent, PEG consists of a mixture of oligomers of different lengths conferring a more 3D structure with increased molecular stability compared with less complex molecules such as BDDE [19,20]. Monticelli et al, observed in their study that the lower effective crosslinker ratio for PEG may be responsible for the different rheological properties compared with BDDE fillers and that the variable swelling rate (speed of water incorporation into the hydrogel network) between the two compounds is closely linked. Lower swelling rates have been reported for PEG as compared with BDDE-based formulations both in vitro and in vivo [21]. Rheologically, it has been shown that PEG - hydrogels display improved elasticity (higher G’) as compared to BDDE HA fillers at the same molar concentrations and that PEG crosslinked HA possess a greater resistance to degradation by hyaluronidase [2].
The HA dermal filler Neauvia Stimulate used in the present study also contains Glycine and L-Proline, two amino acid constituents found in all the types of collagen. Proline is also a major substrate for arginine synthesis which is directly responsible for maintaining normal haemodynamic and nutrient transport through nitric oxide production, while glycine is a key component of ECM proteins elastin and collagen [23].
With the increasing demand for better treatment modalities and better results we are witnessing a growing evolution of products, services, techniques and products. Previously, dermal fillers were injected in order to replace volume lost naturally by the aging process. Recent technological developments have focused on dermal regeneration and skin quality. We have seen this with dermal fillers attributed to producing collagen through a direct transduction mechanism of fibroblast stretching. Such dermal fillers include hyaluronic acid-based or poly-L-lactic acid-based products that have shown to have potential fibrotic foreign body reaction/granuloma formation [13,24].
Neauvia dermal fillers were used in both patients presented in this paper. All Neauvia dermal fillers that use PEG crosslinking technology to stabilize the HA acid chains have shown to have a high safety profile. It has been shown to have a very low risk of immune-mediated adverse effects, particularly granulomatous reaction and associated cellulitic processes [19]. Rauso R et. Al. in their 2021 paper: Clinical Experience with PEGylated Hyaluronic Acid Fillers: A 3-year Retrospective Study state how an interesting feature of the PEGylation process is the total absence, up to now, of foreign body reaction or granulomas related to these fillers. Also in the present case series, no side effects related to immunogenicity were detected, further solidifying the benefits of PEG crosslinked HA fillers [25].
Kubik P et al. Examined the potential use of PEG crosslinked HA fillers in their study entitled Evaluation of the Safety of Neauvia Stimulate Injectable Product in Patients with Autoimmune Thyroid Diseases Based on Histopathological Examinations and Retrospective Analysis of Medical Records. They observed that the limitation of the recognition and presentation of antigens, expressed in a statistically significant decrease in the number of CD4+ and CD8+ T cells in the immediate vicinity of the introduced product, shown in prospective histopathological studies in patients suffering from Hashimoto’s disease, is the basis for the safety of PEGylated hyaluronic acid fillers They state that from the perspective of immunological mechanisms, the subsequent statistically significant reduction in the presence of B lymphocytes as well as monocytes and macrophages is most likely the result of reducing the activity of T lymphocytes [26]. Their findings can be considered critically important in the world of aesthetic dermal filler treatments since autoimmune diseases such as Hashimoto Thyroiditis (HT) are may no longer contraindicated for HA dermal fillers that are PEG crosslinked. This can be considered significant since the incidence of this disease is estimated to be 0.8 per 1000 per year in men and 3.5 per 1000 per year in women [27].
Another benefit of using Neauvia Stimulate dermal filler is the CaHA component which further adds to the skin rejuvenation process by synergistically stimulating fibroblast collagen production, providing support for newly formed collagen, increasing elastin and proteoglycan concentrations, ECM remodelling without inducing an immunologic response and neoangiogenesis. Furthermore, the addition of amino acids glycine and proline to this dermal filler add a beneficial effect of providing the building blocks for collagen synthesis [13,28,29].
In this paper we presented two middle aged female patients who presented to our clinic due to the typical first signs of aging; skin laxity, drooping malar regions, thinning skin, skin blemishes, nasolabial fold crease, decreased skin hydration and overall dissatisfaction regarding their appearance. Following treatment using a combination of different Neauvia PEG crosslinked dermal fillers, we saw a visual improvement in all areas. Most importantly, the patients showed more contentment regarding their appearance and skin quality, increasing their self-esteem and confidence.
Conclusion
True tissue regeneration and subsequently the best aesthetic results for our patients cannot be achieved by focusing one treatment modality alone. We are familiar with the multifactorial concepts and mechanisms associated with skin remodelling and regeneration. It is imperative that aesthetic medicine physicians recognize the complexity and dynamic approach that each patient requires. Isolated treatments that influence only precise points in the homeostatic/regenerative process result in only limited outcomes. These are frequently associated with unfavourable or mediocre results and generally dissatisfied patients. Therefore, it is crucial that physicians choose products that address all the factors associated with aging and migrate away from risky products that can elicit a fibrotic-chronic inflammatory foreign body response by choosing products with a high safety profile.
Declarations
Availability of data and materials: The data presented in this publication are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Financial support and sponsorship: None.
Conflicts of interest: The author declare no conflicts of interest.
Ethical approval and consent to participate: Not applicable. Medical documentation analysis. The study was conducted in accordance with the Declaration of Helsinki.
Consent for publication: Informed consent was obtained from the subject involved in the report. Written informed consent has been obtained from the patients to publish this paper.
References
- Bravo BSF, de Almeida TSC, Carvalho RM, Machado CJ, Bravo LG, et al. Dermal Thickness Increase and Aesthetic Improvement with Hybrid Product Combining Hyaluronic Acid and Calcium Hydroxyapatite: A Clinical and Sonographic Analysis. Plast Reconstr Surg Glob Open. 2023; 11(6): e5055. doi: 10.1097/GOX.0000000000005055.
- Attenello NH, Maas CS. Injectable fillers: Review of material and properties. Facial Plast Surg. 2015; 31(1): 29-34. doi: 10.1055/s0035-1544924.
- Casabona G, Kaye KO. Invited discussion on: Combining calcium hydroxylapatite and hyaluronic acid fillers for aesthetic indications: Efficacy of an innovative hybrid filler. Aesthetic Plast Surg. 2022; 46: 382-384.
- De Almeida AT, Figueredo V, da Cunha ALG, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (Radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019; 7: e2160.
- Moradi A, Shirazi A, David R. Nonsurgical Chin and Jawline Augmentation using calcium hydroxylapatite and hyaluronic acid fillers. Facial Plastic Surg FPS. 2019; 35(2): 140-148. doi: 10.1055/s0039-1683854.
- Edsman K, Nord LI, Ohrlund A, Lärkner H, Kenne AH. Gel properties of hyaluronic acid dermal fillers. Dermatol Surg 2012; 38: 1170-1179.
- Kadouch JA. Calcium hydroxylapatite: A review on safety and complications. J Cosmet Dermatol. 2017; 16: 152-161.
- Fakih-Gomez N, Kadouch J. Combining Calcium Hydroxylapatite and Hyaluronic Acid Fillers for Aesthetic Indications: Efficacy of an Innovative Hybrid Filler. Aesthetic Plast Surg. 2022; 46(1): 373-381. doi: 10.1007/s00266-021-02479-x.
- Yag-Howard C, DeNigris J. Novel filler technique: Hyaluronic acid and calcium hydroxylapatite mixture resulting in favorable esthetic and longevity outcomes. Int J Womens Dermatol. 2021; 7: 817-819.
- Neuber F. Fat grafting. Cuir Kongr Verh Otsum Ges Chir. 1893; 20: 66.
- Kablik J, Monheit GD, Yu L, Chang G, Gershkovich J. Comparative physical properties of hyaluronic acid dermal fillers. Dermatol Surg. 2009; 35: 302-312.
- Felix Bravo B, Bezerra de Menezes Penedo L, de Melo Carvalho R, Amante Miot H, Calomeni Elias M. Improvement of Facial Skin Laxity by a Combined Technique With Hyaluronic Acid and Calcium Hydroxylapatite Fillers: A Clinical and Ultrasonography Analysis. J Drugs Dermatol. 2022; 21(1): 102-106. doi: 10.36849/JDD.2022.6333.
- Corduff N. Introducing aesthetic regenerative scaffolds: An immunological perspective. J Cosmet Dermatol. 2023; 22(1): 8-14. doi: 10.1111/jocd.15702.
- Lorenc ZP, Bass LM, Fitzgerald R, Goldberg DJ, Graivier MH. Physiochemical Characteristics of Calcium Hydroxylapatite (CaHA) Aesthet. Surg. J. 2018; 38: S8-S12. doi: 10.1093/asj/sjy011.
- Zerbinati N, D’Este E, De Silvestri A, Zullino M, Rabbiosi G, et al. Efficacy of Pegylated Hyaluronic Acid Filler Enriched with Calcium Hydroxyapatite: A 24-Week Post-Market, Observational, Prospective, Open-Label, Single-Center Study. J Funct Biomater. 2023; 14(7): 345. doi: 10.3390/jfb14070345.
- Zerbinati N, Esposito C, Cipolla G, Calligaro A, Monticelli D, et al. Chemical and mechanical characterization of hyaluronic acid hydrogel cross-linked with polyethylen glycol and its use in dermatology. Dermatol. Ther. 2020; 33: e13747. doi: 10.1111/dth.13747.
- Zerbinati N, Sommatis S, Maccario C, Capillo MC, Grimaldi G, et al. Toward physicochemical and rheological characterization of different injectable hyaluronic acid dermal fillers cross-linked with polyethylene glycol diglycidyl ether. Polymers. 2021; 13: 948. doi: 10.3390/polym13060948.
- Cassuto D, Bellia G, Schiraldi C. An Overview of Soft Tissue Fillers for Cosmetic Dermatology: From Filling to Regenerative Medicine. Clin Cosmet Investig Dermatol. 2021; 14: 1857-1866. doi: 10.2147/CCID.S276676.
- Marino F, Cosentino M, Legnaro M, Luini A, Sigova J, et al. Immune profile of hyaluronic acid hydrogel polyethylene glycol crosslinked: An in vitro evaluation in human polymorph nuclear leukocytes. Dermatol Ther. 2020; 33(3): e13388. doi: 10.1111/dth.13388.
- Zerbinati N, Capillo MC, Sommatis S, Maccario C, Alonci G, et al. Rheological Investigation as Tool to Assess Physicochemical Stability of a Hyaluronic Acid Dermal Filler Cross-Linked with Polyethylene Glycol Diglycidyl Ether and Containing Calcium Hydroxyapatite, Glycine and L-Proline. Gels. 2022; 8(5): 264. doi: 10.3390/gels8050264.
- Monticelli D, Martina V, Mocchi R, et al. Chemical characterization of hydrogels crosslinked with polyethylene glycol for soft tissue augmentation. Open Access Maced J Med Sci. 2019; 7: 1077-1081. doi: 10.3889/oamjms.2019.279.
- Lee HY, Jeong SH, Baek JU, Song JH, Kim HE. Mechanical improvement of Hyaluronic Acid (HA) hydrogels and incorporation of Polyethylene Glycol (PEG). Archiv Neurol. 2001; 58: 1105-1109. doi: 10.1001/archneur.58.7.1105.
- Scarano A, Rapone B, Amuso D, Inchingolo F, Lorusso F. Hyaluronic Acid Fillers Enriched with Glycine and Proline in Eyebrow Augmentation Procedure. Aesthetic Plast Surg. 2022; 46(1): 419-428. doi: 10.1007/s00266-021-02412-2.
- Trinh LN, Gupta A. Non-Hyaluronic Acid Fillers for Midface Augmentation: A Systematic Review. Facial Plast Surg. 2021; 37(4): 536-542. doi: 10.1055/s-0041-1725164.
- Rauso R, Nicoletti GF, Bove P, Rauso GM, Fragola R, et al. Clinical Experience with PEGylated Hyaluronic Acid Fillers: A 3-year Retrospective Study. Open Access Maced J Med Sci. 2021; 9(B): 1168-73.
- Kubik P, Gallo D, Tanda ML, Jankau J, Rauso R, et al. Evaluation of the Safety of Neauvia Stimulate Injectable Product in Patients with Autoimmune Thyroid Diseases Based on Histopathological Examinations and Retrospective Analysis of Medical Records. Gels. 2023; 9(6): 440. doi: 10.3390/gels9060440.
- Mincer DL, Jialal I. Hashimoto Thyroiditis. In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing. 2023. PMID: 29083758.
- UrdialesGálvez F, Braz A, Cavallini M. Facial rejuvenation with the new hybrid filler HArmonyCa™: Clinical and aesthetic outcomes assessed by 2D and 3D photographs, ultrasound, and elastography. J Cosmet Dermatol. 2023; 22(8): 2186-2197. doi: 10.1111/jocd.15706.
- Yutskovskaya Y, Kogan E, Leshunov E. A randomized, split-face, histomorphologic study comparing a volumetric calcium hydroxylapatite and a hyaluronic acid-based dermal filler. J Drugs Dermatol. 2014; 13(9): 1047-52.