
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 4
Unveiling Sjogren’s syndrome: A clinical case of nodular pulmonary amyloidosis
Hassan Aljaziri*; Ali Alsehiw; Hani Almohammedali; Mohammed Alsaleh; Abdulaziz Almulhim
Department of Radiology, King Fahad Hospital Hofuf, Saudi Arabia.
*Corresponding Author: Hassan Aljaziri
Department of Radiology, King Fahad Hospital Hofuf, Saudi Arabia.
Email: drjaziri1@gmail.com
Received : Nov 20, 2024
Accepted : Dec 16, 2024
Published : Dec 23, 2024
Archived : www.jclinmedimages.org
Copyright : © Aljaziri H (2023).
Abstract
Sjögren’s Syndrome (SS) is rarely associated with pulmonary manifestations, including Nodular Pulmonary Amyloidosis (NPA), a condition often identified incidentally during imaging. Amyloidosis involves the buildup of abnormal proteins in different forms and the most common form in SS with lung involvement is light-chain (AL) Amyloidosis. We present the case of a 45-year-old woman with SS who had a persistent cough, breathlessness, dry mouth, and dry eyes. Imaging revealed incidental finding of lung nodules and cystic changes within lung parenchyma, indicating amyloid involvement with Lymphocytic Interstadial Pneumonia (LIP). This case underscores the importance of considering pulmonary amyloidosis when lung abnormalities including of pulmonary nodules and cystic changes are found in SS patients.
Keywords: Sjögren’s syndrome; Pulmonary nodules; Amyloidosis; Nodular amyloidosis.
Citation: Aljaziri H, Alsehiw A, Almohammedali H, Alsaleh M, Almulhim A. Unveiling Sjogren’s syndrome: A clinical case of nodular pulmonary amyloidosis. Open J Clin Med Images. 2024; 4(2): 1197.
Introduction
Amyloidosis occurs when misfolded proteins accumulate in organs, impairing their function. Amyloidosis classified based on the composition type of the fibrils, the light-chain (AL) Amyloidosis is the most common type affecting the lungs, leading to nodules, however, other fibril types are not common to affect lung like reactive (AA) Amyloidosis and hereditary types [1,2].
Sjögren’s Syndrome (SS) defined as chronic systemic autoimmune disorder primarily targeting exocrine glands, frequently presents with sicca symptoms such as dry mouth and eyes. While lung involvement is less common in Sjögren’s Syndrome (SS), it can include conditions like interstitial lung disease and amyloid deposits. Pulmonary amyloidosis in SS is often found incidentally during imaging [2,3].
Case presentations
A 45-year-old female presented with progressive dyspnea and a persistent dry cough for over two months. Her medical history included xerostomia and xerophthalmia managed with artificial tears.
She also reported intermittent joint pain without associated systemic symptoms such as fever or weight loss. Physical examination revealed stable vital signs and unremarkable respiratory findings.
Laboratory investigations were notable for a significantly elevated Antinuclear Antibody (ANA) titer of 1:1280, while other parameters, including complete blood count and metabolic profiles, were within normal limits.
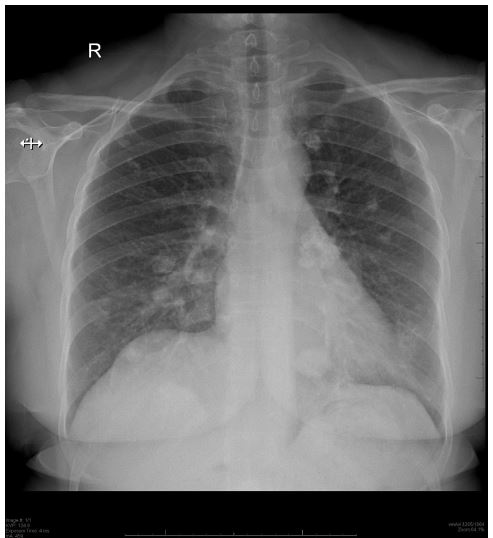
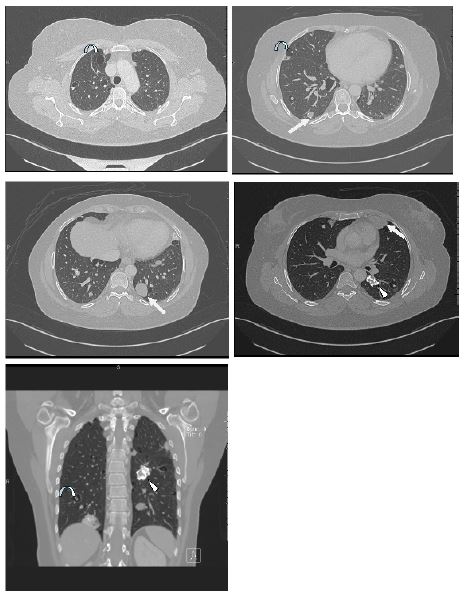
Imaging investigation began with a chest x-ray which shows multiple nodular opacities bilaterally (Figure 1). High-Resolution Computed Tomography (HRCT) identified randomly distributed pulmonary nodules of varying sizes, some exhibiting calcification, alongside thin-walled cystic lesions predominantly located adjacent to vascular structures (Figure 2).
Discussion
Pulmonary abnormalities are detected in up to one-third of asymptomatic patients with Sjogren’s Syndrome (SS). These abnormalities can range from incidental radiological findings to significant clinical conditions such as Interstitial Lung Disease (ILD) or Non-Specific Interstitial Pneumonia (NSIP) [4-6].
Although amyloidosis rarely affects the lung parenchyma in SS, it typically results in localized nodular deposits within the lungs, unlike systemic amyloidosis, which impacts multiple organs. AL amyloidosis is the most common subtype in pulmonary presentations, characterized by multiple irregular nodules, sometimes with calcifications. Conversely, AA amyloidosis is usually linked to chronic inflammatory diseases and systemic involvement. According to Spencer’s classification, our case corresponds to type 2 pulmonary amyloidosis. Spencer categorized pulmonary amyloidosis into three types: (Type 1) tracheobronchial amyloidosis, (Type 2) nodular parenchymal amyloidosis, and (Type 3) diffuse parenchymal amyloidosis, which can be either interstitial or diffuse alveolar septal amyloidosis [2,7].
A review of the literature shows that pulmonary amyloidosis nodules in SS vary in size from one cm to four cm in diameter. These nodules are often discovered incidentally on chest radiographs of asymptomatic patients with other conditions. In SS-associated amyloidosis, the nodules are generally large, irregular, randomly distributed, smooth-bordered, and frequently calcified. Diffuse nodular amyloidosis is the most common radiological pattern and may appear alone or with cysts of various sizes, similar to Lymphocytic Interstitial Pneumonia (LIP), which is often associated with pulmonary nodules. The differential diagnosis of pulmonary nodules in SS patients should include amyloidosis, tuberculosis, abnormal lymphocyte proliferation (lymphoma), and endemic fungal infections [6,8].
This case report highlights a rare association between nodular pulmonary amyloidosis and Sjogren’s Syndrome (SS). While the underlying mechanisms of autoimmune diseases and associated inflammation often explain systemic amyloidosis, single-organ amyloidosis is rare. Further research is needed to understand the mechanisms behind amyloid deposition in autoimmune diseases, particularly in isolated organs.
Conclusion
This report underscores a rare presentation of Sjogren’s Syndrome (SS) with nodular pulmonary amyloidosis and associated Lymphocytic Interstitial Pneumonia (LIP). It emphasizes the importance of considering localized pulmonary amyloidosis in the differential diagnosis for SS patients presenting with diffuse nodules.
References
- Pepys MB. Amyloidosis. In: Weatherall DJ, Ledingham JGG, Warrell DA, editors. Oxford Textbook of Medicine. 3rd ed. Oxford: Oxford University Press. 1995; 1512-24.
- Rajagopala S, Singh N, Gupta A, et al. Pulmonary amyloidosis in Sjögren’s syndrome: A case report and systematic review of the literature. Respirology. 2010; 15(6): 860-6.
- Ito I, Nagai S, Kitaichi M, et al. Pulmonary manifestations of primary Sjögren’s syndrome: A clinical, radiologic, and pathologic study. Am J Respir Crit Care Med. 2005; 171(6): 632-8.
- Franquet T, Gimenez A, Monill JM, et al. Primary Sjögren’s syndrome and associated lung disease: CT findings in 50 patients. AJR Am J Roentgenol. 1997; 169(3): 655-8.
- Jeong YJ, Lee KS, Chung MP, et al. Amyloidosis and lymphoproliferative disease in Sjögren syndrome: Thin-section computed tomography findings and histopathologic comparisons. J Comput Assist Tomogr. 2004; 28(6): 776-81.
- Okamura H, Tsukamoto H, Kumamoto T, et al. Pulmonary amyloidosis in Sjögren’s syndrome: A case report and review of the literature. Respir Med Case Rep. 2021; 34: 101516. doi:10.1016/j.rmcr.2021.101516.
- Westermark P, Johansson B, Natvig JB. Senile cardiac amyloidosis: A clinical and histopathological study. Pathol Res Pract. 1979; 165(1-3): 111-21. doi:10.1016/S0344-0338(79)80058-8.
- Hui AN, Koss MN, Hochholzer L, et al. Amyloidosis presenting in the lower respiratory tract. Clinicopathologic, radiologic, immunohistochemical, and histochemical studies on 48 cases. Arch Pathol Lab Med. 1986; 110: 212-8.