
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 5
Folliculotropic mycosis fungoides in a patient with human immunodeficiency virus: A case report
Mariana Sousa Certal*; Rita G Cunha; Mariana NA Silva; Marta S Barrigas; Sandra MG Tavares
Department of Internal Medicine, Unidade Local de Saúde (ULS) de Trás-os-Montes e Alto Douro, Portugal.
*Corresponding Author: Mariana Sousa Certal
Department of Internal Medicine, Unidade Local de Saúde (ULS) de Trás-os-Montes e Alto Douro, Avenida da Noruega, 5000-508, Vila Real, Portugal.
Email: marianacertal@gmail.com
Received : Dec 05, 2024
Accepted : Jan 06, 2025
Published : Jan 13, 2025
Archived : www.jclinmedimages.org
Copyright : © Sousa Certal M (2025).
Abstract
Mycosis fungoides, a cutaneous T-cell lymphoma, has different subtypes. The most common subtype is folliculotropic mycosis fungoides. Although the folliculotropic mycosis fungoides etiology is not fully known, the association with type 1 immunodeficiency virus is scarcely described. The authors present a case of a 41-year-old male infected with Human Immunodeficiency virus type 1, who exhibited erythematous lesions on the upper arms and trunk. A biopsy confirmed the diagnosis of folliculotropic mycosis fungoides. The patient was treated with topical corticosteroids, resulting in a positive outcome. Understanding the clinical spectrum of mycosis fungoides is crucial for accurate diagnosis.
Keywords: Mycosis fungoides; Human immunodeficiency virus; Cutaneous lymphoma.
Citation: Sousa Certal M, Cunha RG, Silva MNA, Barrigas MS, Tavares SMG. Folliculotropic mycosis fungoides in a patient with human immunodeficiency virus: A case report. Open J Clin Med Images. 2025; 5(1): 1199.
Introduction
Mycosis Fungoides (MF) is the most common Cutaneous T Cell Lymphoma (CTCL), representing almost 50% of all primary cutaneous lymphomas [1,2]. Clinically, classic MF presents with erythematous patches that may evolve into infiltrated plaques [2,3]. Folliculotropic Mycosis Fungoides (FMF) is the most prevalent subtype of MF in adults, accounting for approximately 10% of cases [1,2,4]. Histopathologically, it is characterized by folliculotropic infiltrates surrounding the hair follicles [1,2,5]. The clinical presentation is variable and can include patches, plaques, nodules, acneiform lesions, comedones, cysts, alopecia, and prurigo-like nodules [1,6]. The etiology of FMF is not entirely understood [1]. Although some studies suggest a possible viral etiopathogenesis of MF, particularly involving Human T-cell Lymphotropic Virus type I (HTLV-I) and Human Immunodeficiency Virus (HIV), these associations are rare and the FMF subtype in HIV-positive patients has not been reported yet [7,8]. FMF was previously considered to have a worse prognosis than classical MF [1,6], however, recent studies indicate that FMF can be divided into two prognostically distinct subtypes, one of which has a better prognosis, similar to early-stage MF [4,5,9]. The authors describe a case involving an HIV-positive patient with a mild form of FMF.
Case report
A 41-year-old man presented for his first Internal Medicine consultation after transferring from another hospital. He reported pruritus and erythematous lesions that had developed over the past nine months. His medical history included a nine-year history of HIV-1 infection, acquired through heterosexual contact, and treated with antiretroviral drugs (Emtricitabine 200 mg daily, Tenofovir 245 mg daily, and Darunavir 600 mg twice daily). He had no history of acquired immunodeficiency syndrome-defining conditions. Previous blood tests and nadir CD4+ count were unavailable. Currently, his HIV viral load is undetectable, and his CD4+ count is 42 cells/mm³ (7%). He has been smoking 20 cigarettes per day for the past 20 years. His current regimen includes the same antiretrovirals, with ritonavir 100 mg twice daily added as a booster, and Trimethoprim/sulfamethoxazole 400/80 mg daily for Pneumocystis jirovecii prophylaxis. There are no other relevant past medical history or malignancies, and no family history of disease.
On examination, the patient was in good general condition, weighing 72 kg with a body mass index of 27.5 kg/m². He was afebrile, without cyanosis, breathing comfortably, and had normal cardiac and pulmonary auscultation. He exhibited multiple erythematous-violaceous lesions with adherent desquamation, not psoriasiform, showing a hyperpigmented, atrophic appearance with parched areas, located on the upper arms, interclavicular, and infra-auricular regions (Figures 1a & 1b).
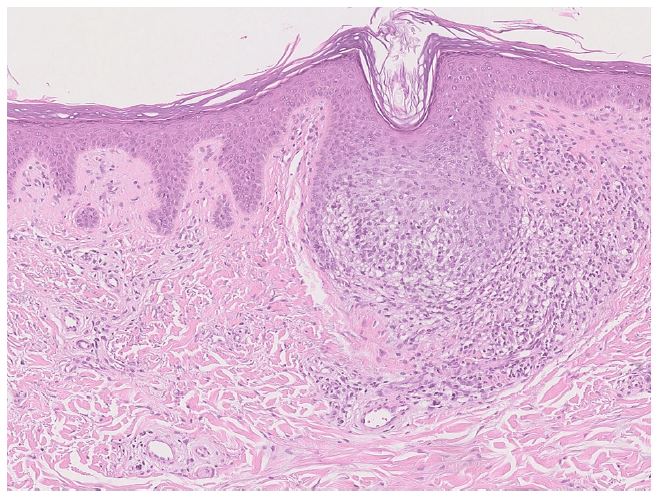
The conjunctivae were not injected, and oral mucous membranes were moist. No lymphadenopathy was noted. Blood tests showed relative lymphopenia (470/μl) and hyperlipidemia (total cholesterol 220 mg/dL, triglycerides 233 mg/dL). CMV and HTLV serologies were negative, and Epstein-Barr Virus serology indicated a past infection. Non-contrast CT showed no abnormalities. A skin biopsy of the right forearm revealed perifollicular and perieccrine lymphocytic infiltrate, follicular epithelium infiltration by inflammatory lymphocytes, nuclear irregularities, and some mucin deposits (Figure 2). The patient responded well to topical corticosteroids (Methylprednisolone aceponate 1 mg/g) applied intermittently for 4 months.

Discussion
Mycosis Fungoides (MF) is the most prevalent T-cell lymphoma, characterized by the proliferation of T lymphocytes [3]. There are 3 distinct clinicopathologic variants of MF: Folliculotropic MF (FMF), pagetoid reticulosis, and granulomatous slack skin [3]. FMF, one of these subtypes, primarily affects adults and males, following an indolent course that progresses from patches to infiltrative plaques and eventually tumors over several years or decades [1,3,10].
FMF has a broad clinical spectrum but usually manifests in cutaneous sites rich in pilosebaceous units [6]. The classical presentation includes indurated, scaly, hairless erythematous patches, plaques, or tumors. These plaques are often associated with alopecia, comedones, and erythematous follicular papules [9]. Other manifestations can include grouped follicular papules and cystic lesions [6]. Unlike classical MF, FMF patients with FMF experience severe pruritus in advanced stages [6,9]. Although FMF lesions commonly appear on the head and neck, initial lesions usually occur on the trunk, with advanced cases affecting the head and neck [1,9].
Histopathologically, FMF is characterized by a dense inflammatory infiltrate with hyperchromatic cells featuring cerebriform nuclei, affecting the follicular epithelium while sparing the epidermis [1]. Mucin deposits and perieccrine infiltrates may also be presented [9]. Five pathologic patterns have been described, which can occur independently or concomitantly: mucinous deposits in the follicular unit, granulomatous reaction with follicular epithelium destruction, eosinophilic folliculitis-like presentation, cystic and comedonal changes, and basaloid folliculolymphoid hyperplasia with folliculotropism [5]. The immunophenotype is similar to that classic MF, with a predominance of atypical CD4+ and CD3+ cells that ares CD8- [1,3,6]. Additionally, CD8+, CD30+ variants or small clusters of CD20+ are not uncommon [11]. The exact etiology and mechanisms by which neoplastic T cells are attracted to follicular units remain unclear [6].
HIV-1 infection predisposes individuals to lymphomas, primarily aggressive B-cell types, while cutaneous T-cell lymphomas are rarely reported in this context. FMF in HIV-infected patients is not well-documented, and T-cell lymphomas in these individuals are often linked to severe immunodeficiency and low survival rates [8].
Previously, FMF was considered to have a worse prognosis and lower survival rates. However, recent studies suggest otherwise. FMF can be categorized into two patterns with different prognostic implications: an early/indolent variant with a 5-year survival rate of 92%, and an advanced/aggressive variant with a 55% survival rate [1,4,6,9]. The early/indolent FMF is characterized by follicle-based patches on the trunk with superficial infiltrates and an indolent course. In contrast, the advanced/aggressive FMF presents as nodules and tumors on the head and trunk, with more extensive plaques infiltration [1,5,9].
FMF is treated similarly to tumor-stage MF (IIB) due to its deep perifollicular infiltration, which reduces responsiveness to skin-directed therapies. Treatment options include systemic therapies such as PUVA, acitretin, bexarotene, total skin electron beam radiation, romidepsin, and interferon. Advanced cases may require irradiation, allogeneic stem cell transplant, or chemotherapy [6,9]. However, early/indolent FMF may be managed with PUVA phototherapy, potent topical corticosteroids, or local radiation therapy [12,13].
The authors present a case of an HIV-1 seropositive patient with severe immunodeficiency and persistent CD4+ count below 50 cells/mm³. This patient exhibited early/indolent FMF and responded positively to topical corticosteroids, a treatment that has been reported to control disease progression in some cases [4].
Conclusion
Due to its broad clinical spectrum and rarity, diagnosing FMF is particularly challenging and often requires clinicopathologic correlation. Nevertheless, differentiating cutaneous T-cell lymphomas and their variants is crucial, as it significantly affects prognosis and treatment options. This case aims to remind clinicians to consider FMF when evaluating immunocompromised patients with cutaneous lesions.
Conflict of interest: research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Malveira MIB, Pascoal G, Gamonal SBL, Castañon MCMN. Folliculotropic mycosis fungoides: challenging clinical, histopathological and immunohistochemical diagnosis. An Bras Dermatol. 2017; 925: 73-75.
- Kempf W, Zimmermann AK, Mitteldorf C. Cutaneous lymphomas-An update. 2019; 37: 43-47.
- Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005; 105: 3768-3785.
- Kamijo H, Sugaya M. Two distinct variants of mycosis fungoides: Folliculotropic MF and erythrodermic MF. J Dermatol. 2019; 46: 1136-1140.
- Van Santen S, Jansen PM, Quint KD, Vermeer MH, Willemze R. Plaque stage folliculotropic mycosis fungoides: histopathologic features and prognostic factors in a series of 40 patients. J Cutan Pathol. 2020; 47: 241-250.
- Feng H, Beasley J, Meehan S, Liebman TN. Folliculotropic mycosis fungoides. Dermatol Online J. 2018; 2412: 13030-5.
- Gahongayire F. Mycosis fungoides and Sezary syndrome against a human immunodeficiency virus-positive background: case report. Int J Dermatol. 2007; 46: 32-5.
- Burns MK, Cooper KD. Cutaneous T-cell lymphoma associated with HIV infection. J Am Acad Dermatol. 1993; 29: 394-9.
- Mitteldorf C, Stadler R, Sander CA, Kempf W. Folliculotropic mycosis fungoides. J Dtsch Dermatol Ges. 2018; 16: 543-557.
- Uribe-Bojanini E, Santa-Vélez C, Rueda-Cadena X, Morales SD. Severe and Lethal Presentation of Folliculotropic Mycosis Fungoides. Micosis fungoide foliculotropa de presentación grave y letal. Actas Dermosifiliogr. 2019; 110: 412-414.
- Virmani P, Myskowski PL, Pulitzer M. Unusual variants of mycosisfungoides. Diagn Histopathol. 2016; 22: 142-151.
- Hodak E, Amitay-Laish I, Feinmesser M, Davidovici B, David M, et al. Juvenile mycosis fungoides: cutaneous T-cell lymphoma with frequent follicular involvement. J Am Acad Dermatol. 2014; 70: 993-1001.
- Van Santen S, Van Doorn R, Neelis KJ, et al. Recommendations for treatment in folliculotropic mycosis fungoides: report of the Dutch Cutaneous Lymphoma Group. Br J Dermatol. 2017; 177: 223-228.