
Open Journal of Clinical and
Medical Images
Case Report - Open Access, Volume 5
Huge uterine leiomyoma in a 27-year-old nulliparous woman initially misdiagnosed as an ovarian tumor: A case report
Egbal Lutfi Mohamed Salih*
Department of Obstetrics and Gynecology, Sabt Alaya Hospital, Alkhaldiyah, Saudi Arabia.
*Corresponding Author: Salih ELM
Department of Obstetrics and Gynecology, Sabt Alaya Hospital, Alkhaldiyah, Saudi Arabia.
Email: dr.egballutfi2010@gmail.com
Received : Nov 24, 2025
Accepted : Dec 23, 2025
Published : Dec 30, 2025
Archived : www.jclinmedimages.org
Copyright : © Salih ELM (2025).
Abstract
Large uterine leiomyomas may mimic ovarian tumors, particularly in young nulliparous women, leading to diagnostic uncertainty.
Case: We report a 27-year-old nulliparous woman who presented with a massive abdominopelvic mass initially interpreted as a complex ovarian tumor on MRI. Preoperative imaging suggested bilateral ovarian dermoid cysts, but exploratory supra-umbilical laparotomy revealed a giant intramural uterine fibroid.
Conclusion: This case highlights the diagnostic challenges of large pelvic masses and emphasizes the importance of considering leiomyoma in differential diagnoses, even when imaging favors ovarian pathology.
Citation: Salih ELM. Huge uterine leiomyoma in a 27‑year‑old nulliparous woman initially misdiagnosed as an ovarian tumor: A case report. Open J Clin Med Images. 2025; 5(2): 1214.
Introduction
Uterine leiomyomas are the most common benign tumors of the female genital tract. While typically detected incidentally or through symptoms such as abnormal bleeding or pelvic pressure, large leiomyomas may distort pelvic anatomy to the extent that they mimic adnexal masses. Misdiagnosis is especially common in young, nulliparous women where ovarian pathology may be suspected first. We present a case of a huge intramural uterine leiomyoma initially misdiagnosed as an ovarian teratoma based on MRI findings.
Case report
A 27-year-old nulliparous woman presented with progressive abdominal enlargement over one year, associated with pelvic pressure, constipation, and early satiety. Physical examination revealed a firm mass extending above the umbilicus. Tumor markers including CA‑125, AFP, and β‑hCG were within normal limits.
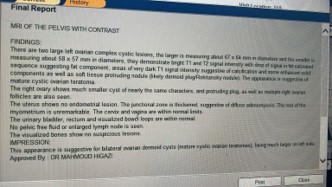
MRI of the pelvis with contrast reported bilateral ovarian dermoid cysts, with the largest measuring approximately 67×64 mm, containing fat and calcification components consistent with mature cystic teratoma. The uterus was described as unremarkable.

During exploratory supra-umbilical laparotomy, however, a giant intramural uterine leiomyoma occupying nearly the entire abdominal cavity was identified. The ovaries and tubes were normal and separate from the mass. Myomectomy was performed successfully, preserving the uterus and adnexa.
Histopathology confirmed a benign uterine leiomyoma with no evidence of sarcomatous change. Postoperative recovery was uneventful, and follow‑up demonstrated full symptomatic relief.
Discussion
Large leiomyomas can present diagnostic challenges when imaging findings overlap with adnexal masses. MRI is generally the preferred modality for characterization of uterine tumors; however, extremely large leiomyomas may distort anatomy, leading to misinterpretation. In this case, the mass effect displaced the uterus posteriorly while mimicking bilateral ovarian dermoid cysts due to heterogeneous signal intensity.
Misdiagnosis may alter preoperative planning and counseling, especially for women desiring fertility preservation. This case underscores the importance of maintaining a broad differential diagnosis and correlating imaging findings with clinical examination.
Supra-umbilical laparotomy was required due to the size and cephalad extension of the mass. Myomectomy remains the preferred option for young women, and in this patient, normal ovaries were confirmed intraoperatively, allowing preservation of reproductive potential.



Conclusion
This case demonstrates that even with modern imaging, large uterine leiomyomas may be misdiagnosed as ovarian tumors. Thorough clinical evaluation, careful interpretation of imaging, and surgical exploration remain essential when the diagnosis is uncertain. Fertility‑preserving surgery should be prioritized in young patients whenever feasible.
References
- Stewart EA. Uterine fibroids. Lancet. 2001; 357: 293–298.
- Fasih N, et al. Leiomyomas of the uterus: understanding the imaging spectrum. Radiographics. 2008; 28: 2031–2048.
- Khan AT, Shehmar M, Gupta JK. Uterine fibroids: current perspectives. Int J Womens Health. 2014; 6: 95–114.
- Murase E, et al. Uterine leiomyomas: histopathologic features, MR imaging findings, differential diagnosis, and treatment. Radiographics. 1999; 19: 1179–1197.